

Bone cancer is cancer that is present in the bone. They can be two main types of bone cancers.
Primary bone cancers are those that have started in the bone and originate in the cells that make up the bone, cartilage, or other cells in the bone. Most of these cancers are sarcomas. Common tumors are Osteosarcomas, Chondrosarcomas, and Ewing’s sarcoma.
Secondary bone cancers are those that have started in other organs in the body such as Lung, Breast, etc, and then spread to the bone.
In this section, we will be talking only about primary bone cancers, and secondary bone cancers are discussed in another section.
A lot of other benign lesions are seen in the bone. These are tumors but not cancers and do not have the capacity to spread to other parts of the body.
There are different types of primary bone Cancers based on the type of cell they start in the bone or cartilage. The common cancers are listed below.
Osteosarcoma or Osteogenic Sarcoma
This is the most common type of bone Cancer that develops in adolescents, teenagers and young adults commonly but can happen at any age. The cancer can occur in any bone in the body but commonly happens around the knee in the femur (thigh bone), tibia (leg bone) and in the shoulder.
Ewing’s Sarcoma
This is a type of Cancer that is more common in children and adults at a younger age but can develop at any age. It most commonly occurs in the pelvis, femur (thigh bone) and tibia (leg bone). This type of sarcoma can also arise from outside the bone in the soft tissues of the body.
Chondrosarcoma
This is a type of bone sarcoma that arises from the cartilage of the bone. The cartilage is the smooth whitish structure present at the and of the bone. It occurs in middle to older age and can occur in any part of the body but common in the upper arm and femur (thigh bone). The other areas it can arise include, pelvis, ribs and bottom of the skull.
Spindle cell Sarcoma
These are sarcomas arising from the bone but are made up of soft tissues and do not have bone forming cells. These occur in older adults and are also called as Malignant fibrous histiocytoma (MFH) or Leiomyosarcoma of the bone or Fibrosarcoma depending on its features. These are rare tumours.
There are some risk factors which can increase the likelihood of getting bone cancers and these are listed here.
Exposure to Radiation
Previous exposure to radiation increases the risk of getting bone cancer.
Benign bone disease
Having certain types of benign bone conditions such as enchondromas, osteochondromas can become cancerous over time.
Genetic Factors
Certain genes that are present in families increase their risk of getting various cancers including bone cancers. One such disease is Li Fraumeni syndrome, where the families with this condition have an increased risk.
Childhood Cancer
Children who had treatment for childhood cancer with chemotherapy and radiotherapy have an increased risk of bone cancers when they grow up as compared to general population who have not had such treatments.
The symptoms produced by bone cancers can vary depending on the type of tumour and the location of the tumour.
Swelling or a lump
This is a common symptom that is seen in these conditions. The swelling can be growing quickly over a few days to weeks or grow slowly over months to years. It can sometimes be a swelling that has been the same size for a long time but starts to grow again. The swelling can be painful or painless. The swelling can be associated with redness of the skin in the area.
Pain
Pain is a common symptom of these lesions but is not a necessary symptom to diagnose a cancer as some can be painless. Commonly, pain is present and worse while resting. Sometimes the pain can be radiating down the arm or leg due to compression of a nerve by the tumour.
Fracture
A fracture of the bone can be a presenting symptom of an underlying bone cancer. The fracture can happen with minimal trauma as the bone is weak in that area. Such a fracture is called a pathological fracture.
Other symptoms
Other symptoms associated with bone cancers include fever, tiredness, reduced appetite and weight.
The following investigations are done to help in the diagnosis of primary bone Cancer.
X-ray
An x-ray of the affected bone is usually the first test done in the diagnosis of bone Cancers. When the patient complains of pain or a swelling related to the bone, an x-ray is done to look for a cause. The appearances on the x-ray can give a good indication of the possible cause.
MRI Scan
An MRI scan of the affected bone is the next mode of investigation and is usually done after an x-ray. An MRI gives significantly more information of the area and is able to identify cancer versus benign swellings in the bone.
CT or PET-CT scan
A CT scan or a PET-CT scan is done to help in the diagnosis of a bone cancer as well as in the staging process. The staging investigation tells us whether there is any spread of the cancer from its site of origin to other parts of the body.
Bone Scan
An Isotope bone scan is done to determine the features of the abnormal areas in the bones. This scan is done only in certain situations.
Biopsy
A biopsy of the suspected area is needed to confirm the presence of a bone cancer. Tests such as MRI can be very good in informing about potential nature of the problem, but a biopsy is usually needed before treatment strategy is planned. The biopsy is done with the guidance of an ultrasound or CT scan. The biopsy should be done carefully in consultation with the operating surgeon as the location of the biopsy is very important. A wrong location could make a difference as to which surgery is done later, either a limb sparing one or an amputation.
Bone marrow biopsy
A biopsy of the bone marrow is done when certain bone cancers such as Ewing’s sarcoma are suspected.
Bone Sarcomas is staged according to the TNM staging or number staging system. TNM stands for tumour, node and metastases. It is as follows. Other staging and classification systems are also present for these cancers but only the TNM system for long bones is spoken of here.
T Stage (for long bones, trunk and Head)
| T1 | Tumour up to 8cm in size |
| T2 | Tumour more than 8 cm in size |
| T3 | T3 Tumour discontinuous in the primary bone site |
N Stage
| N0 | No involvement of lymph nodes from the cancer |
| N1 | Involvement of lymph nodes from the cancer |
M Stage
| M0 | No distant spread of cancer from its original site |
| M1a | Spread of cancer into the Lung |
| M1b | Spread of cancer to other sites |
Grading of Osteosarcoma
Every Osteosarcoma that is diagnosed on biopsy is given a grade from 1 to 3. The grading also plays a role in the staging process.
Grade 1 Well differentiated (low grade)
Grade 2 Moderately differentiated (high grade)
Grade 3 Poorly differentiated (high grade)
Number Staging in Osteosarcoma
| T stage | N Stage | M Stage | Grade | Number |
|---|---|---|---|---|
| T1 | N0 | M0 | 1 | 1A |
| T2 | N0 | M0 | 1 | 1B |
| T3 | N0 | M0 | 1 | 1B |
| T1 | N0 | M0 | 2,3 | 2A |
| T2 | N0 | M0 | 2,3 | 2B |
| T3 | N0 | M0 | 2,3 | 3 |
| Any T | N0 | M1a | Any | 4A |
| Any T | N1 | Any M | Any | 4B |
| Any T | N1 | M1b | Any | 4B |
This is the most common type of bone cancer that develops in adolescents, teenagers and young adults commonly but can happen at any age. The cancer can occur in any bone in the body but commonly happens around the knee in the femur (thigh bone), tibia (leg bone) and in the shoulder.
Treatment of Osteosarcoma
Surgery
The most important treatment for Osteosarcoma is the surgical removal of the cancer. This combined with chemotherapy forms the main part of treatment and combination of the two treatments increase the chances of better control and cure of the disease.
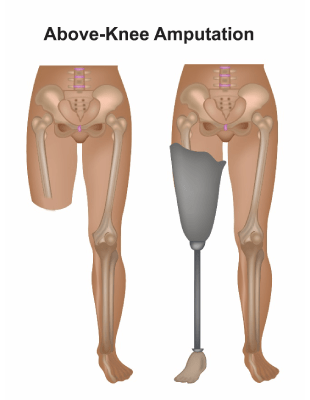
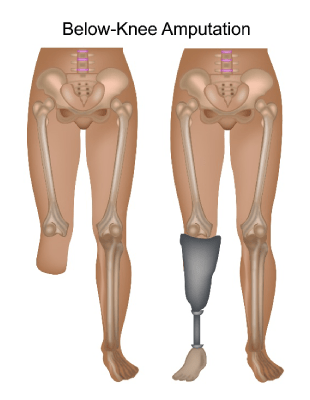
Surgical resection can be an amputation, where the affected limb is removed or a limb sparing option where the tumour is removed with an adequate margin and the limb is spared. Wide resection involves removal of the cancer with surrounding normal tissues without affecting the function of the limb.
If an amputation is done, a whole limb including a neighbouring joint may have to be removed. A prosthesis can be worn afterwards to aid in mobility or other functions of that limb. An amputation is done when the tumour is extensive or is involving important structures around it such as major blood vessels or nerves or recurrence after a limb sparing operation. Side effects of an amputation include phantom pain, where the patient can experience a feeling of pain in a part of the limb that has been removed. This improves over time.
A limb sparing surgery is more commonly done than an amputation. Here a part of the bone in the limb is removed and a prosthesis or a bone from another part of the body is put in to replace the removed bone. The limb is left in place to help with function.
Which operation to select will depend on the location of the cancer, the age of the patient as the bones are still growing in a younger patient, the activity level of the patient such as running etc and the functional outcome after the operation.
Most operations involving primary bone cancers require some sort of reconstructive surgery to account for loss of tissues that are removed at the operation. This reconstructive surgery aims to restore the function of that part of the body in the best possible way. Various types of this surgery include insertion of an endoprosthesis which is a metal or plastic object put in place of the removed bone. The prosthesis helps in restoring function of that limb. The prosthesis is tailor made for the patient so that it fits in exactly for the patient after surgery. In some surgeries a bone graft is needed where a part of the bone is removed from another part of the patient or from another person(allograft). This piece of bone is placed into the defect created by the surgery.
Chemotherapy
Chemotherapy is an important component of treatment in Osteosarcoma to help in cure of the disease. Chemotherapy is given with a combination of drugs and can be given either before (neoadjuvant) or after (adjuvant) the surgery. A lot of times, some chemotherapy is given before and some after the surgery. Common types of chemotherapy used include Methotrexate, Doxorubicin and Cisplatin (MAP) or a combination of Doxorubicin and Cisplatin. Other drugs that can be added to MAP chemotherapy include Ifosfamide and Etoposide.
Patients who have metastatic or stage 4 disease are also given chemotherapy using various combinations of drugs listed above.
Radiotherapy
Osteosarcoma is not very sensitive to radiotherapy and therefore it is not a standard mode of treatment.
Osteosarcoma
Risk factors for osteosarcoma include previous radiotherapy or chemotherapy, usually many years before, (>10 years). In adult patients, those over 40 years of age, presence of benign bone lesions such as Paget’s disease of the bone, fibrous dysplasia, chronic infections of the bone-osteomyelitis or presence of bone infarcts can be risk factors for developing osteosarcoma.
Common symptoms associated with Osteosarcoma include pain in the involved area of the bone which can be present for many months. Along with pain, there may be a swelling over the area which is usually soft and tender to touch.
For details on diagnosis and staging see section on bone tumours.
Radiotherapy can occasionally be used in patients who cannot have surgery or in some types of osteosarcoma (small cell).
Recurrence
Patients who have cancer that has recurred or come back after initial treatment are offered treatment depending on the site of recurrence. The cancer commonly recurs in the lungs. In some patients with recurrence in the lung, surgical removal of that may be possible and could be pursued. This can be combined with chemotherapy before or after the operation. For patients where surgery is not possible, chemotherapy is the option to try and control the disease.
Chondrosarcoma is a cancer that arises from cartilage tissue. Chondrosarcoma can make up about 20% of all primary bone related tumours. The behaviour of chondrosarcomas can vary greatly from being a very slow growing tumour in low grade ones to an aggressive tumour in high grade cancers. Most chondrosarcomas, up to 90% are low to intermediate grade and slow growing. Unlike Ewing’s sarcoma and Osteosarcomas, Chondrosarcomas mostly occur in people over the age of 50. Commonly involved bones include the femur (thigh bone), the pelvis and humerus (arm bone).
Symptoms associated with Chondrosarcoma include pain and swelling in the bones, swelling on or close to a bone that is growing slowly over weeks or months. Occasionally, patients may notice a swelling that has been present for a long time and has started to increase rapidly.
Treatment of Chondrosarcoma
Treatment of Chondrosarcoma is based on the size, location, grade and stage of tumour at the time of diagnosis.
Surgery
Surgical treatment is the only option that will enable a cure for Chondrosarcoma. The type of surgery done is variable depending on the tumour.
For low grade tumours, intralesional curettage is commonly done. This involves curetting the tumour from the involved bone and using additional treatment like injection of bone cement or cryotherapy. This is a less aggressive approach and does not need any reconstructive surgery.
For intermediate and high-grade tumours, complete removal of the cancer is done by wide excision. This is usually associated with reconstructive surgery to get the best possible functional outcome in that the patient is able to function as much as prior to the operation.
Radiotherapy
Radiotherapy is used as a treatment in patients with high grade chondrosarcoma, especially when it has been incompletely removed or it cannot be removed by surgery because of its location in the body. The radiotherapy is given once a day, 5 days a week for at least 6 weeks. Usually standard external beam radiotherapy is given but Proton beam radiotherapy is a good option for cancers that are deep seated in the body. For those patients with metastatic or stage 4 chondrosarcomas, palliative radiotherapy lasting 1-10 treatments is used to control symptoms.
Chemotherapy
For patients diagnosed with stage 4 disease, chemotherapy may be used to help control the disease. Drugs sued include Cisplatin and Doxorubicin.
This is a type of cancer that is more common in children and adults at a younger age but can develop at any age. It most commonly occurs in the pelvis, femur (thigh bone) and tibia (leg bone). This type of sarcoma can also arise from outside the bone in the soft tissues of the body and all of these together are called as Ewing’s family of tumours.
Symptoms in Ewing’s Sarcoma
Common symptoms in patients with Ewing’s sarcoma include pain and swelling in the bone or joint that is involved, reduced mobility in the limb. Other symptoms include fever, sweats in the night, reduced appetite and weight loss. Other specific symptoms depend on the place of origin of the cancer.
Treatment of Ewing’s Sarcoma
Treatment options for Ewing’s sarcoma include chemotherapy, surgery and radiotherapy and these are listed below.
Chemotherapy
This is usually the first treatment that is considered in this condition. It is a combination of drugs and is part of a multi-modality approach that includes surgery, radiotherapy or both. The drugs used include Vincristine, Ifosfamide, Doxorubicin, Etoposide, Cyclofosfamide. This treatment is intensive and given for about 3 months prior to surgery. Chemotherapy has a good chance of reduction of the cancer prior to the operation. This treatment is given along with G-CSF support which will help quicker recovery of white blood cells. Common side effects of chemotherapy include tiredness, nausea, vomiting, low blood counts, risk of infection and bleeding, hair loss, loose motions, constipation. Chemotherapy is given again after completion of surgery or radiotherapy or both depending on which treatment is selected. Up to 6 months of chemotherapy is considered in total.
Surgery
Surgery forms an important component of treatment for Ewing’s sarcoma. This combined with chemotherapy forms the main treatment in most patients and combination of the two treatments increase the chances of better control and cure of the disease.
Surgical resection can be an amputation, where the affected limb is removed or a limb sparing option where the tumour is removed with an adequate margin and the limb is spared. Wide resection involves removal of the cancer with surrounding normal tissues without affecting the function of the limb.
If an amputation is done, a whole limb including a neighbouring joint may have to be removed. A prosthesis can be worn afterwards to aid in mobility or other functions of that limb. An amputation is done when the tumour is extensive or is involving important structures around it such as major blood vessels or nerves or recurrence after a limb sparing operation. Side effects of an amputation include phantom pain, where the patient can experience a feeling of pain in a part of the limb that has been removed. This improves over time.
A limb sparing surgery is more commonly done than an amputation. Here a part of the bone in the limb is removed and a prosthesis or a bone from another part of the body is put in to replace the removed bone. The limb is left in place to help with function.
Which operation to select will depend on the location of the cancer, the age of the patient as the bones are still growing in a younger patient, the activity level of the patient such as running etc and the functional outcome after the operation.
Most operations involving primary bone cancers require some sort of reconstructive surgery to account for loss of tissues that are removed at the operation. This reconstructive surgery aims to restore the function of that part of the body in the best possible way. Various types of this surgery include insertion of an endoprosthesis which is a metal or plastic object put in place of the removed bone. The prosthesis helps in restoring function of that limb. The prosthesis is tailor made for the patient so that it fits in exactly for the patient after surgery. In some surgeries a bone graft is needed where a part of the bone is removed from another part of the patient or from another person(allograft). This piece of bone is placed into the defect created by the surgery.
Radiotherapy
Radiotherapy is used commonly in patients with Ewing’s sarcoma when surgery is not possible or when surgery along with chemotherapy is unable to achieve clear margins after surgery. Ewing’s sarcoma can occur in any part of the body and some of the cancers cannot be removed by an operation because of their location, for example in the neck, bottom of the skull, abdomen or chest. In these situations, a course of radiotherapy is given in between courses of chemotherapy or after. Radiotherapy, when used, is given daily for 5-6 weeks to the area that is affected.
Treatment of metastatic disease
Metastatic disease is stage 4 disease where the cancer has spread from its place of origin to other parts of the body. In patients with stage 4 Ewing’s sarcoma who are fit enough to have chemotherapy are given chemotherapy with the above described drugs. Other options such as surgery and radiotherapy may be added if it is felt that good control of disease can be achieved with these approaches. Treatment options in this stage are very patient specific and decisions will be made based on the condition of the patient, extent of the disease, the wishes and the financial condition of the patient.
These are tumours or lesions seen in the bone but are not cancers. As they are not cancers, they do not spread to other parts of the body. They can remain static or grow slowly at the place of origin. Benign tumours are commonly found by chance when tests are done for other reasons. In some instances, they cause symptoms. Most of these tumours are managed by serial x-rays or scans over a period of time. Those causing symptoms may need treating. Common tumours are listed below.
Bone forming benign bone Tumours
- Osteoid Osteoma
- Osteoblastoma
Cartilage forming benign bone Tumours
- Osteochondroma
- Enchondroma
- Chondromyxoid fibroma
- Chondroblastoma
Fibrous Tumours
- Fibrous dysplasia
- Ossifying fibroma
Cyst forming Tumours
- Aneurysmal Bone Cyst
Others
Giant cell tumour of the bone
This is a benign tumour of the bone but can spread locally causing symptoms. It is seen in young people and is usually present around the knee. Most of these tumours are managed by surgery in the form of a curettage and bone cement is injected into the area after the surgery. For larger lesions, more aggressive surgery may be needed. For tumours that are not operable or recur after surgery treatment with a drug called Denosumab or use of radiotherapy is done. Very occasionally, these tumours may spread to the lungs.
