

Head and cancers are cancers that start in the head and neck areas. The areas in the head and neck region from where cancers develop include
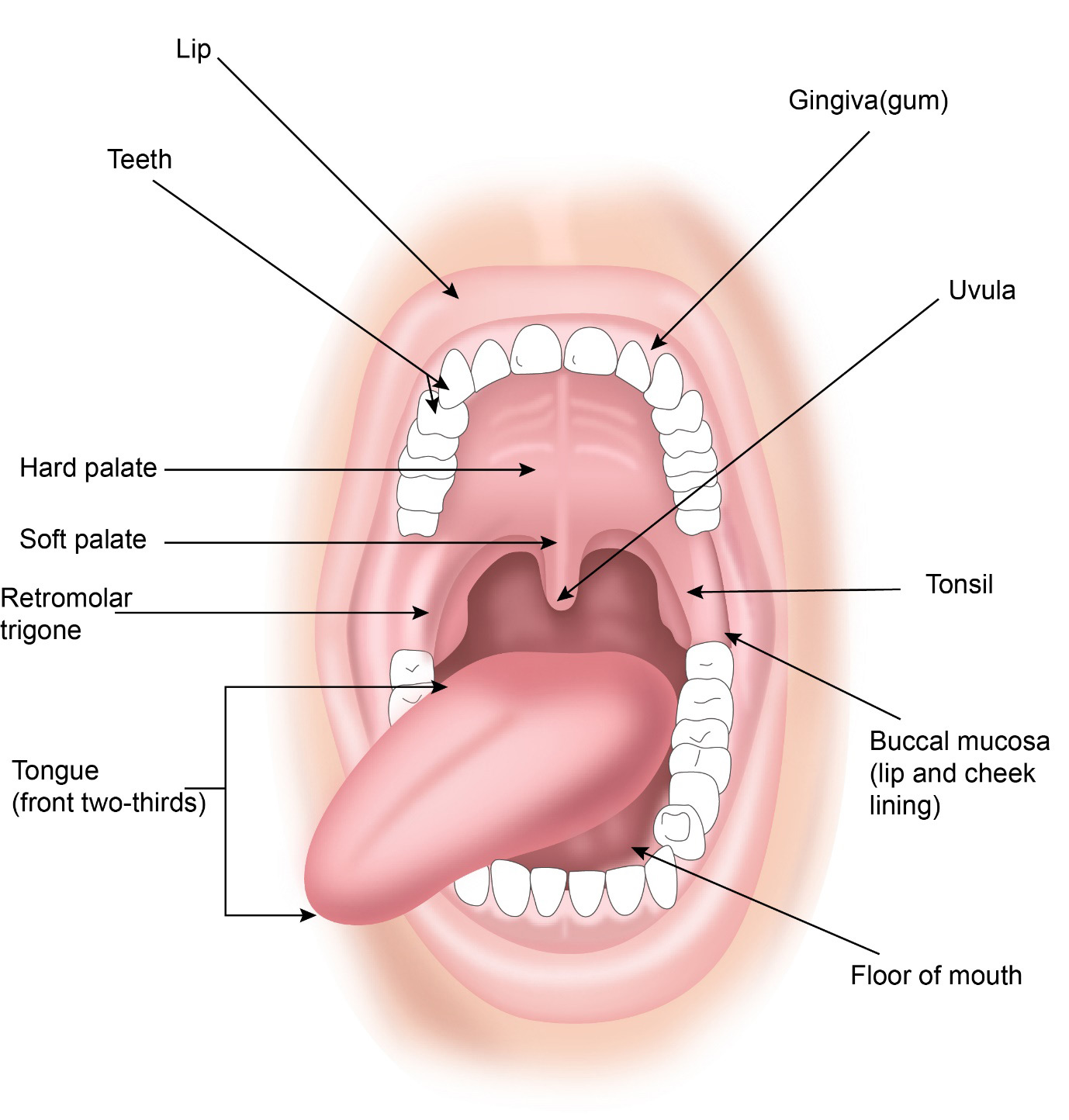
Lip, Tongue, Floor of mouth, Retromolar trigone, Cheek, Roof of mouth
Tonsil, Base of Tongue,
Throat and Voice box
Nasal cavity and Sinuses
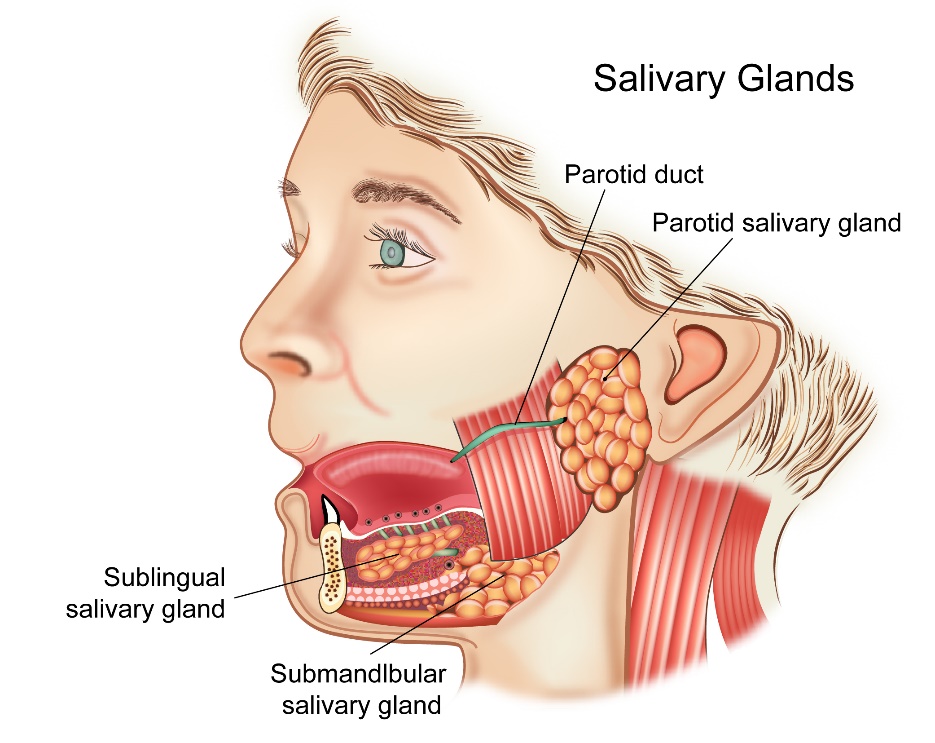
Tumours arising from the salivary glands including the parotid gland, submandibular gland, sublingual gland and other minor salivary glands in the mouth
Area behind the nose
Most head and neck cancers are squamous cell carcinomas. Tumors arising from the salivary glands include pleomorphic adenoma, mucoepidermoid carcinoma, adenoid cystic carcinoma, adenocarcinoma, etc. Other tumors arising in the head and neck region include lymphoma, sarcomas, and neuroblastomas.
According to Globocan data 2018, there were nearly 205,000 cancers of the head and neck area making up about 17% of all cancers. Of these cancers, those of the lip and oral cavity (in the mouth) account for about 58%. This is because of the high use of tobacco chewing and smoking particularly chewing.

Pre-cancerous conditions are those that could develop into a cancer over time. Pre-cancerous conditions in the head and neck region include leukoplakia, erythroplakia or leukoerythroplakia. These are white, red or reddish white patches present in the mouth which can turn into cancer over time. Other conditions include squamous hyperplasia or dysplasia. If these lesions are found, close observation is needed to look for changes and to enable prompt treatment.
Head and Neck cancers can be classified based on their site of origin and are listed below
Cancers of the oral cavity
The cancers in this group include those that start on the lip, inside of the cheek, tongue, floor of the mouth, roof of the mouth, retromolar trigone (area behind the last molar teeth) and gums.
Cancers of Nose and paranasal Sinuses
These are cancers that are in the nose and the sinuses that are present around the nose
Cancers of the Pharynx
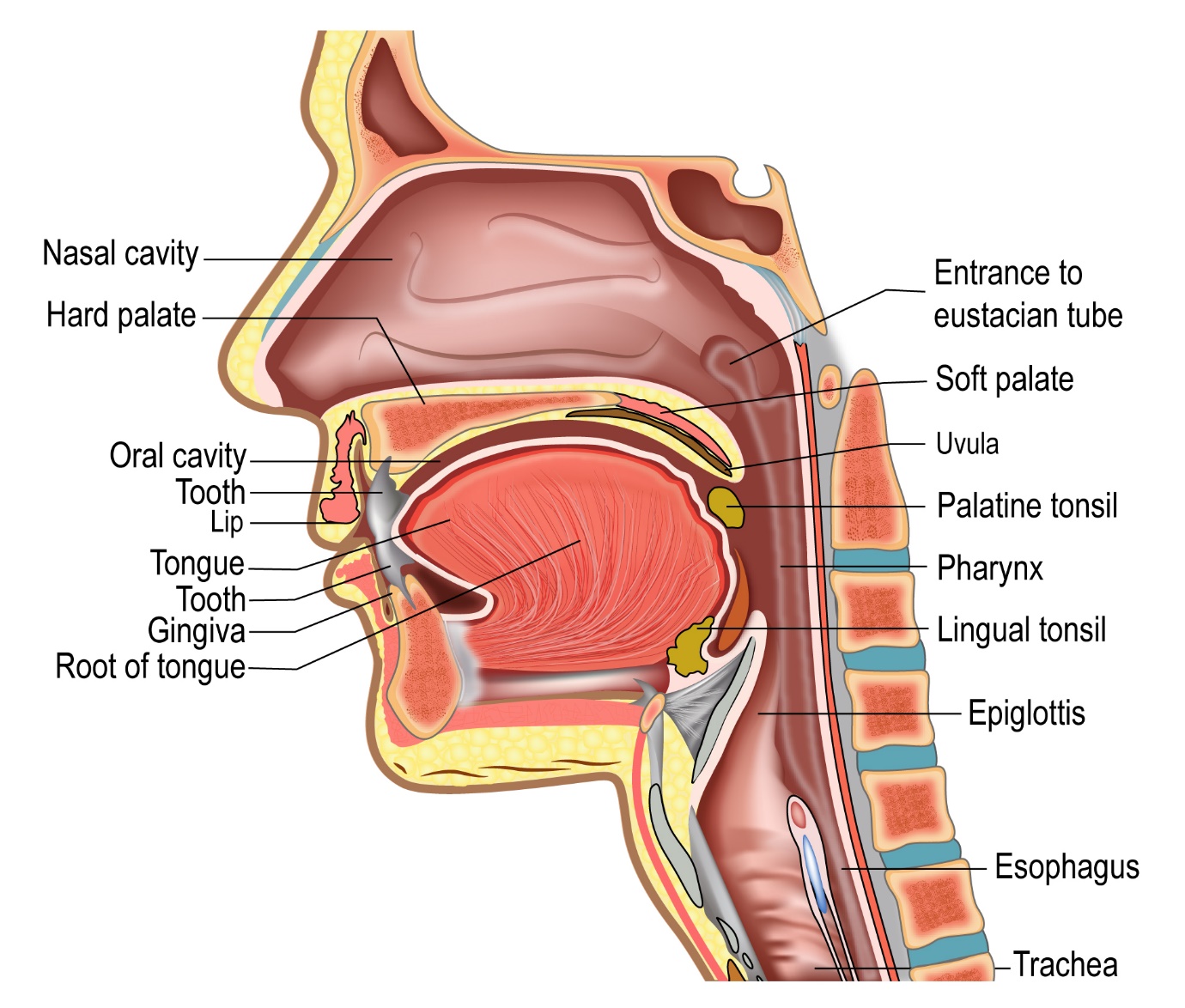
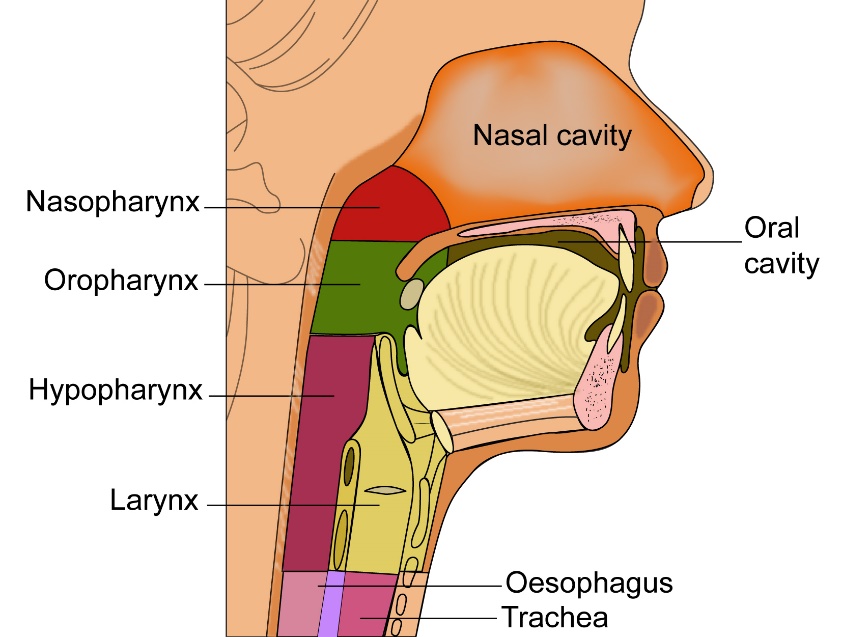
The pharynx is the area of the head and neck that is behind the nasal cavity, mouth and the voice box. The pharynx can be divided into nasopharynx, which is the pharynx behind the nasal cavity,
The oropharynx is the pharynx that is behind the mouth and the hypopharynx is the area behind the voice box or larynx.
Cancer that arises in the nasopharynx is called as nasopharyngeal cancer. Cancers that arise from the oropharynx include those from the tonsils, tongue base and soft palate.
Cancers starting in the hypopharynx are called as hypopharyngeal cancers.
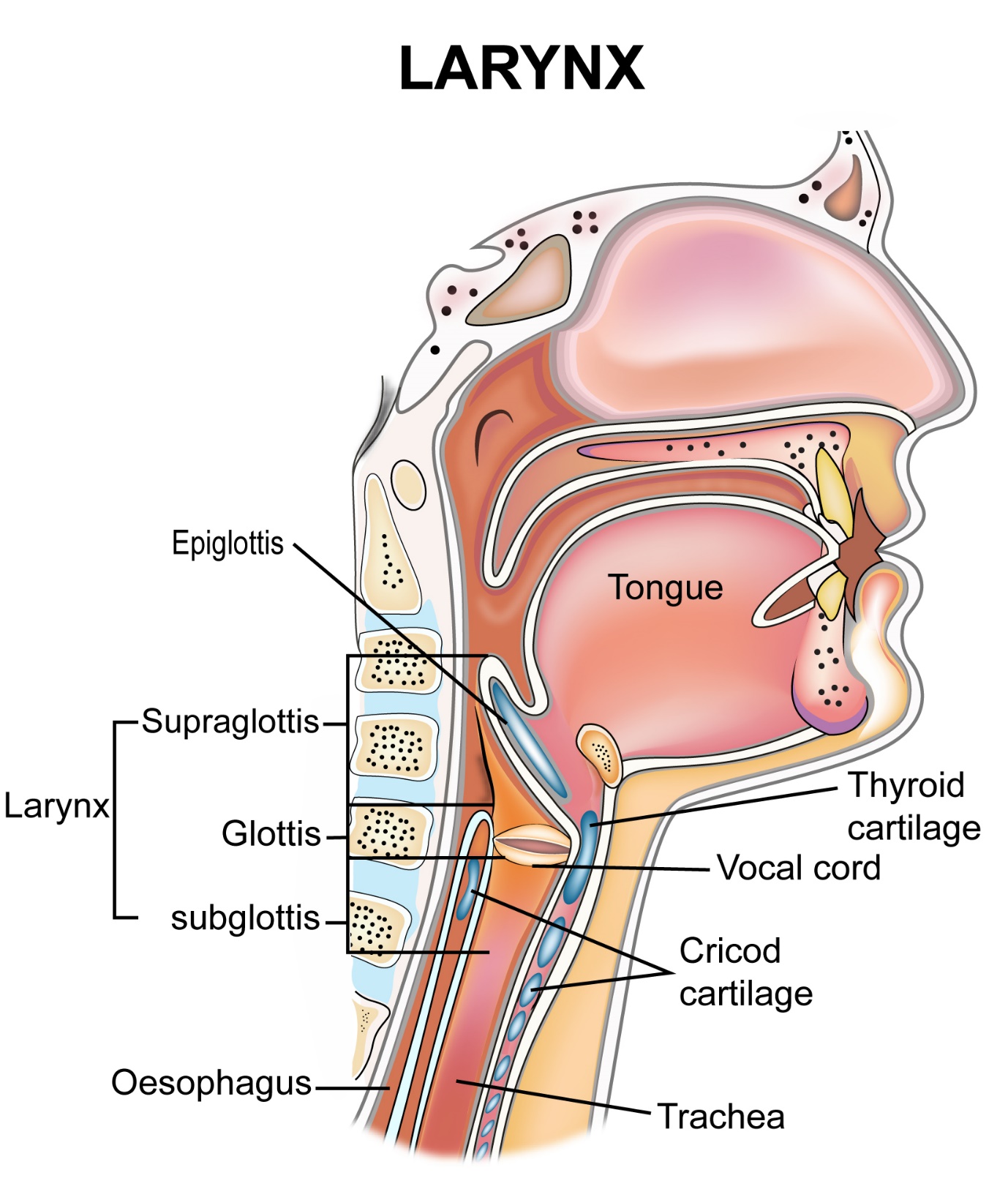
Cancers of the Larynx
The larynx or the voice box is the area in the throat involved with production of voice. Cancers originating from that area are called as laryngeal cancers.
Salivary gland Tumours
Salivary glands produce saliva into the mouth. There are three major salivary glands called parotid, submandibular and sublingual gland present around the mouth. There are also multiple minor salivary glands present around the mouth. Tumours arising from these salivary glands are called as salivary gland tumours. These tumours can be benign or malignant.
Head and neck cancers can also be classified by the types of cells seen in the cancer and these are given below.
Squamous cell Carcinomas
These are by far the most common head and neck cancers and are seen in most sites that are described above.
Others
The other types of cancers seen in this area include lymphomas, sarcomas, adenocarcinomas, melanomas and benign tumours.
Most cancers that develop in the head and neck region have common causes and risk factors which are listed below.
Smoking
Smoking is one of the biggest risk factors for head and neck cancer. This can be smoking a cigarette, beedi, pipe or a cigar. Smoking increases the risk of head and neck cancer by 5 to 25 times as compared to non-smokers. Duration of smoking as well as intensity of smoking directly contribute to the risk. Being exposed to second hand smoke may also play a role.
Alcohol
Consumption of alcohol is an important risk factor for the development of head and neck cancer. Consuming significant amount of alcohol increases the risk of head and neck cancer by about 5-10 times when compared to non drinkers. Smoking and alcohol consumption together have a multiplying effect in the development of head and neck cancer.
Viral Infections
HPV
Infection with Human Papilloma (HPV) virus is a risk factor in the development of head and neck cancer. HPV is a sexually transmitted virus and is responsible for other cancers also such as cervical, anal, vaginal and vulval cancers. This virus particularly causes tonsil and base of tongue cancers.
Epstein Barr Virus(EBV)
Epstein barr virus is said to be responsible for the development of nasopharyngeal cancer. This is not sexually transmitted. Nasopharyngeal cancer is not that common in India, but very common in south east asia and china.
Betel Nut Chewing
Betel nut chewing is a very important risk factor and causative agent in the development of head and neck cancer in India and south asia. This chewing can be in the form of pan, gutkha, pan masala and others. This habit mainly causes cancers of the mouth and throat. When betel nut chewing is done with tobacco smoking and alcohol, it has a multiplicating effect in increasing the risk of head and neck cancer.
Diet
A poor diet and a diet low in fruit and vegetables can increase the risk of development of some head and neck cancers.
Others
People exposed to wood dust, those working in the leather industry or those exposed to chemicals such as formaldehyde and mineral oils have a risk of cancers in the nasal cavity and paranasal sinuses.
Head and neck cancers can produce the following symptoms. It is important to note that although these symptoms may represent cancer, a lot of times these symptoms may be due to causes other than cancer. It is still important to visit a doctor if these symptoms persist.
Lump in the Neck
A lump in the neck is a very common symptom associated with head and neck cancer. Patients notice that the lump increases in size over a period of time. This lump is usually due to an enlarged lymph node after spread of cancer into the node.
Lump or swelling in the mouth
Patients with a cancer of the oral cavity(mouth) may notice a lump or swelling in the mouth either on the tongue, lip jaw, cheek etc. An ulcer like area that does not heal may also be a presenting symptom of a cancer in the mouth.
Change in Voice
A change in voice or hoarseness of voice can be a symptom of a cancer in the throat or voice box.
Ear ache or reduced hearing
Having a persistent ache in the ear or onset of reduced hearing in one ear can be a symptom of cancer in the head and neck region.
Cough, breathlessness or difficulty in swallowing
Symptoms such as a persistent cough or difficulty in swallowing can be symptoms of head and neck cancers. Feeling short of breath can also be a symptom.
Nasal Obstruction, bleeding from nose or reduced smell
These symptoms can occur in patients who have cancers in the nasal cavity or nasal sinuses.
Bleeding and Pain
Bleeding and pain are common symptoms with head and neck cancers from all sites.
Others
Patients with advanced head and neck cancers can have symptoms of weight loss, reduced appetite, bleeding, pain, coughing up of blood and tiredness.
The following investigations are done when a head and neck cancer is suspected.
FNA of Neck Mass or Lump
If a neck mass is found that is suspicious for a head and neck cancer, an FNA is done to determine the nature of the mass. FNA helps in identifying the type of lesion, whether benign or malignant. An FNA can be done with the help of an ultrasound scan. It is easy to do and a report is available quickly. In dedicated clinics, an FNA is reported instantly.
Biopsy
A core biopsy involves removing a larger piece of tissue for looking under the microscope than an FNA. This procedure may involve the need for local or general anaesthesia. A core biopsy is done on a suspicious mass in the head and neck area, from where the cancer is felt to have originated.
A core biopsy takes a few days to be reported on.
Examination under Anaesthesia (EUA)
In patients where a primary site of cancer is not seen, an examination of the head and neck area under general anaesthesia is done to identify the source of the cancer. During this procedure an endoscope is passed into the throat, nose and oesophagus if needed to make a diagnosis.
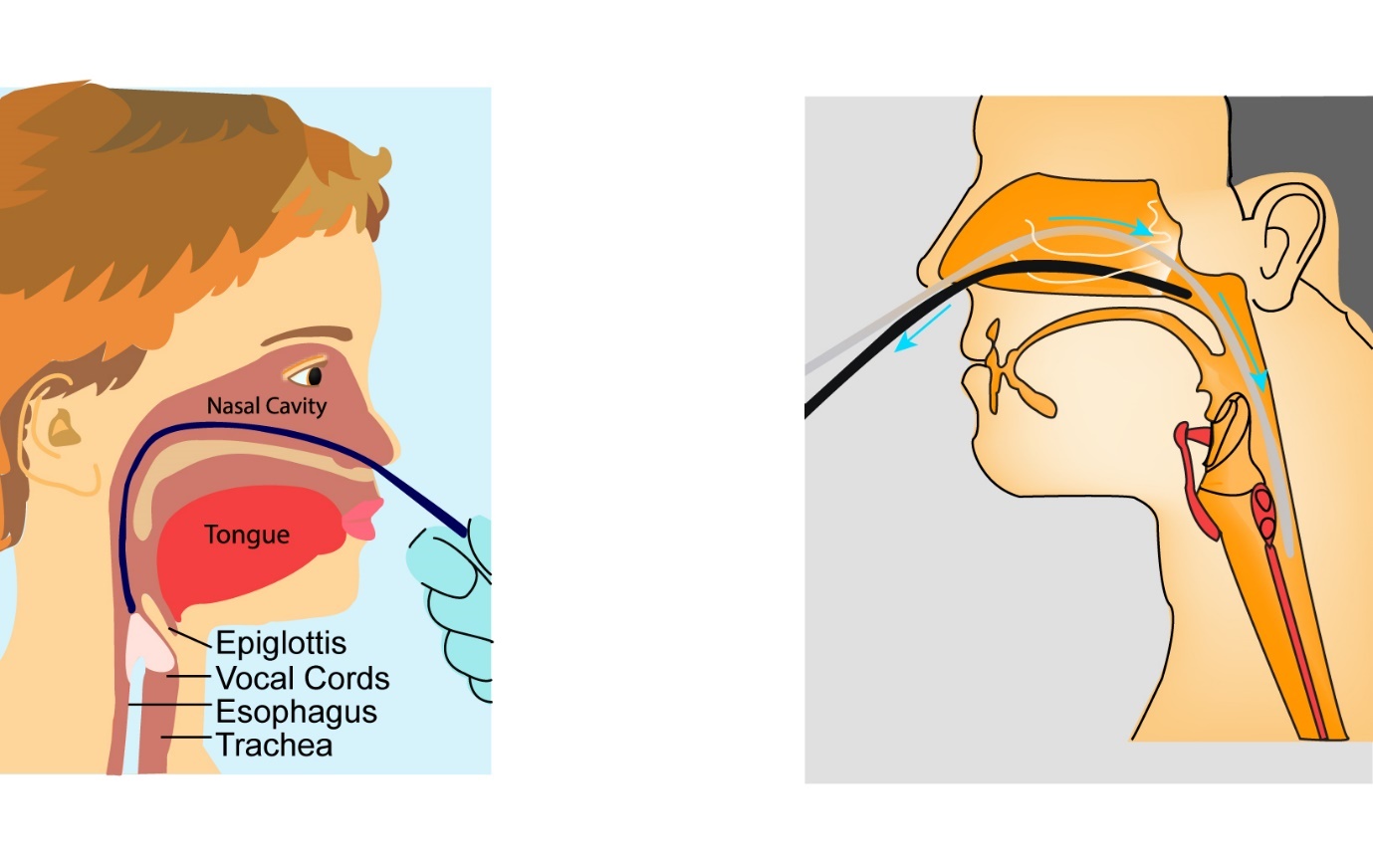
Flexible Nasendoscopy
A flexible nasendoscopy is used to look inside the nose and throat in patients with suspicion of a head and neck cancer. A nasendoscope is a thin flexible tube with a camera at the end of it. It is inserted into the nose and passed into the throat for the doctor to have a look inside. A local anaesthetic spray is used before the procedure.
CT scan
A CT scan of the head and neck region is done to look for a cancer of the head and neck region when there is a suspicion and to look for spread of that cancer and to stage it.
MRI Scan
An MRI scan is done to look for suspected cancer and enlarged lymph nodes and to stage the cancer. Usually either a CT scan or an MRI scan is enough for staging but occasionally both are needed in some situations.
PET CT scan
In some head and neck cancers, enlarged lymph nodes in the neck show cancer but a primary site of origin is not found. A PET CT scan is done in this situation to help locate the site of origin of cancer that has spread to the lymph nodes. This scan helps in accurately getting a stage for the cancer and helps in planning radiotherapy if that treatment option is used.
General Principles
The treatment options for head and neck cancers can be very complex and usually taken by a multi- disciplinary team involving the head and neck Surgical oncologist, Radiation oncologist, Medical oncologist, Radiologist, Pathologist, Plastic surgeons, the Patient and their families and others.
Together, they decide on the best course of action in each patient.
Treatment options for these cancers include surgical removal of the cancer, radiotherapy, chemoradiotherapy, a combination of these treatments and in very advanced cancers, palliative chemotherapy.
Which treatment option to select depends on factors which include
The location of the primary tumour
The spread of tumour to the neighbouring structures from its primary site
The involvement or risk of involvement of lymph nodes in the neck
The functional outcome after the proposed treatment
Spread of cancer to areas in the body other than the head and neck region
The detailed treatment options for each site are listed separately
Surgery in Head and Neck Cancers
Surgery in head and neck cancers involves removal of the cancer at its site of origin as well as removal of the lymph nodes in the neck in most cases. Removal of the cancer at the primary site involves cutting out the cancer and an area of normal cells around the cancer to ensure that all the cancer has been taken out. If the cancer involves structures such as muscle or bone, they are also removed along with the tumour to ensure completeness of resection.
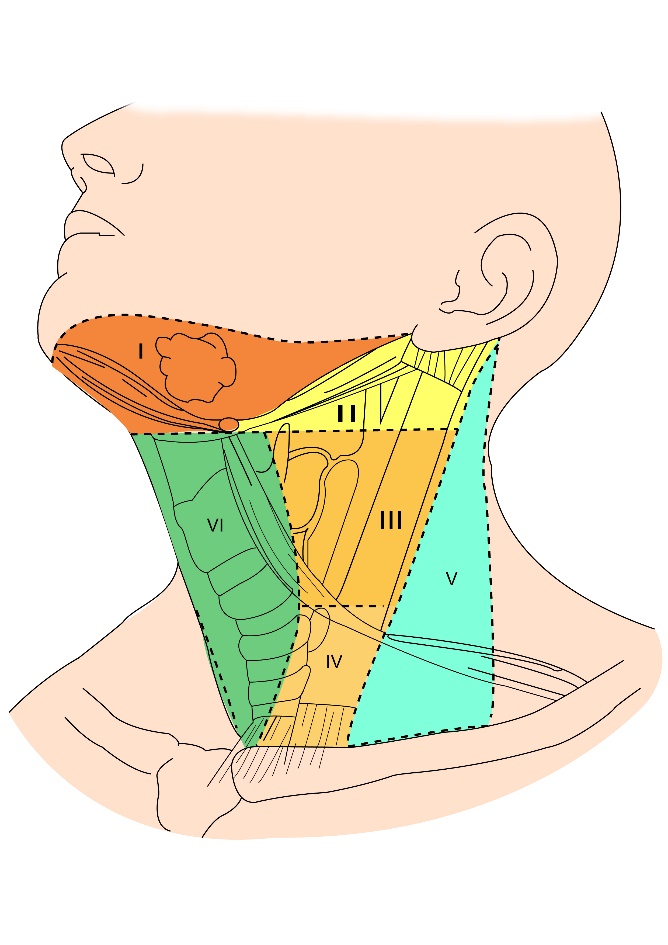
Lymph node Dissection
The lymph nodes in the neck are usually the first places for head and neck cancers to spread to and removal of the lymph nodes ensures removal of any cancer cells that may have moved from their site of origin. The lymph nodes in the neck are divided into 6 levels and the levels that are removed at surgery is determined by the location and type of cancer. This surgery is called as neck dissection. A neck dissection can be on one side of the neck or both sides. This is dependent on the type of cancer and its location.
Types of Lymph node dissection
There are different types of neck dissection done and these are listed below.
Radical Neck Dissection
A Radical neck dissection involves removal of all lymph nodes in the neck as well as removal of other structures in the neck called the internal jugular vein, the sternocleidomastoid muscle and the accessory nerve.
Modified radical neck dissection
A modified radical neck dissection involves removal of all lymph nodes in the neck but only removal of one or more of the following structures of internal jugular vein, sternocleidomastoid muscle and accessory nerve and not all three.
Selective Neck Dissection
A selective neck dissection involves removal of only some lymph nodes in the neck like levels 1-3 and levels 2-4 etc. This type of surgery is done commonly and the selection of lymph nodes to remove depends on the type of cancer and its stage.
Reconstructive Surgery
Reconstructive surgery is commonly used in surgical treatment of head and neck cancers. Important structures in the head and neck region such as tongue, throat, other parts of the mouth, tonsil etc are removed at surgery to get rid of the cancer. Complex reconstructive surgery is needed to correct the defect caused by the surgery and restore function that the removed organ used to do.
This type of surgery is done using skin, muscle, bone from other parts of the body and using them to cover areas that have been removed. Flaps are tissues removed from one part of the body and placed in another. Flaps can be taken from the abdomen, back and arms.
Radiotherapy
Radiotherapy is a very important component of treatment of Head and Neck cancer. Apart from surgery, it is the only curative option.
In head and neck cancer, radiotherapy can be given in two ways
External beam radiotherapy is where the treatment is given with a machine from outside the body and high energy x-rays are delivered to the area of interest
Brachytherapy where a radioactive source is inserted into the area of interest to deliver radiotherapy locally.
Overall, external beam radiotherapy is used most commonly in treating these tumours and brachytherapy is used for early cancers and in some centres only.
This topic will discuss external beam radiotherapy only.
Radiotherapy can be given on its own or as a combination with chemotherapy when it is known as chemoradiotherapy. Radiotherapy or chemoradiotherapy can be used after surgery or instead of surgery.
Radiotherapy is given as a number of fractions. A fraction is radiotherapy treatment given over one sitting. Treatment is usually over 6-7 weeks, daily for 5 days a week.
The treatment area includes the primary tumour area as well as lymph nodes in the neck that contain the cancer or at risk of containing the cancer. One side or both sides of the neck may be treated depending on the site of tumour and its location. Radiotherapy does produce side effects and some general side effects are listed below.
Methods of Radiotherapy
Definitive Radiotherapy or Chemoradiotherapy
This type of treatment is given when radiotherapy or chemoradiotherapy is used as a definitive treatment to cure the patient from the cancer. In such an instance, surgery is not used, and radiotherapy will be the main treatment. Surgery may not be used for various reasons including that the patient is not fit or does not want an operation, surgery is not practically possible in that situation or will be associated with a lot of side effects or will provide a worse functional outcome than radiotherapy.
Adjuvant Radiotherapy or Chemoradiotherapy
In this setting, radiotherapy or chemoradiotherapy is used after surgery. Surgery will remove the main cancer and the lymph nodes. Radiotherapy or a combination of radiotherapy and chemotherapy is used to maximise the chances of cure. In head and neck cancer, this is used when the cancer is large, the margins at the surgery contain cancer or the cancer is very close to the margin. Other factors include spread of cancer outside the lymph nodes in the neck (extracapsular extension), involvement of lymph nodes by the cancer and spread of cancer into the blood vessels or nerves in the area (vascular or perineural invasion).
Palliative Radiotherapy
This type of treatment is used to control symptoms of the cancer when the cancer is not curable any more. The duration of radiotherapy can range from 1 day to 6 weeks depending on the situation.
Side Effects of Radiotherapy
Skin changes
Radiotherapy causes redness and soreness of the skin in the area that it is being given to. The redness starts in a few weeks after start of treatment and peaks a week after the end of treatment.
Redness can be associated with peeling of dry skin. This can be associated with pain and managed with pain killers.
Sore mouth and throat
These symptoms are seen when the area of mouth and throat are treated. Soreness starts after a few days-weeks of treatment and can cause pain on swallowing or chewing food. Symptoms can be managed with medications and modifying diet with eating less spicy and soft food.
Change in voice
These symptoms are seen in patients having radiotherapy to the throat. The voice will improve a few weeks after radiotherapy is finished.
Difficulty eating and drinking
These symptoms are common, and measures are taken before start of treatment in some patients.
Difficulty in eating can start a few weeks into treatment. Measures to help with continuing to eat include using good pain killers, placement of a nasogastric tube which is a thin tube inserted into the stomach through the nose and throat or placement of a PEG tube into the stomach through the skin to help with feeding.
These tubes can be removed once the patient manages to eat normally again.
Dry Mouth
Having a dry mouth after radiotherapy of the head and neck area is common. The amount of dryness depends on the area treated. Constant wetting of the mouth with sips of liquids or use of some medications may be needed in the long term after treatment.
Chemotherapy, biological therapy and Immunotherapy
Chemotherapy
In head and neck cancer, chemotherapy is used as part of chemoradiotherapy or on its own in advanced disease. Chemotherapy drugs commonly used include cisplatin, carboplatin, docetaxel, paclitaxel, 5-Fluorouracil and a biological agent called cetuximab. Immunotherapy is used as a treatment in advanced stage 4 head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors.
Chemotherapy with Radiotherapy (Chemoradiotherapy)
A combination of chemotherapy and radiotherapy is used in head and neck cancers to improve the chances of cure as compared to radiotherapy alone. Here, radiotherapy is the main component of treatment and adding chemotherapy increases the effect of it. Chemoradiotherapy is used in advanced head and neck cancers only as the benefit is limited in early head and neck cancers.
Chemotherapy commonly used with radiotherapy in chemoradiotherapy is a drug called Cisplatin. Some patients may have Carboplatin instead of Cisplatin. This drug is given once a week during the 6-7 weeks of radiotherapy that is used. Cisplatin takes almost 6-8 hours to be given and the patient will need a set of blood tests before every dose of treatment to make sure it is ok to give the treatment. Patients should be healthy enough to have chemoradiotherapy and its benefit is not established for those over the age of 70 years. In these situations, radiotherapy alone is used.
Neo adjuvant Chemotherapy
In this situation, chemotherapy is given before surgery or radiotherapy to reduce the cancer which may enable better removal of cancer at surgery or radiotherapy. Commonly, a combination of 2-3 drugs are used here and treatment is given for 2-3 months. In the three-drug combination Docetaxel, Cisplatin and Fluorouracil are used. In the two-drug combination Cisplatin and Fluorouracil are usually used. Neoadjuvant chemotherapy is used only in some types of head and neck cancers.
Palliative Chemotherapy
Here chemotherapy is used to control the cancer in a situation where cure is not possible. Drugs used here include Cisplatin, Carboplatin, Docetaxel, Paclitaxel, Gemcitabine and Fluorouracil. Chemotherapy can be given as a combination of drugs or as single drugs depending on the fitness of the patient. Chemotherapy may also be given along with Cetuximab, which is a biological agent as described below.
Biological Therapy
Biological therapy is the use of drugs targeting specific areas in the cancer cell. Cetuximab is one such drug which targets the EGFR receptor. It is a monoclonal antibody against this receptor. Cetuximab is given as an infusion into the vein and can be used along with radiotherapy in patients who cannot take chemoradiotherapy. Cetuximab is also used in combination with palliative chemotherapy in stage 4 head and neck cancer patients.
Side effects of Cetuximab can be less than those of chemotherapy and include skin rash, acne, nail changes, sore mouth, loose motions, tiredness, nausea vomiting and abdominal pain among others.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer.
Checkpoint Inhibitors
Immunotherapy is use of drugs that alter how the immune system in the body works. This type of treatment has been used in some cancers for a long time, but newer immunotherapy drugs like checkpoint inhibitors have shown more promise and are being used more often in a number of cancers including head and neck cancer.
In simplistic terms, the newer immunotherapy drugs called checkpoint inhibitors are antibodies against PD-1 or PD-L1 receptors. These receptors are useful in helping the cancer cell to be identified by the body’s immune system (T Cells) as a friend and prevents the immune system from killing the cancer cells. Cancers can produce more of these receptors and will be able to evade the immune system of the body. By using the antibodies against PD-1 and PD-L1, there is a block of this pathway and this enables the body’s immune system to attack the cancer cells and kill them.
As of now, this therapy is used in stage 4 head and neck cancers where the cancer has spread to different parts of the body and the aim of treatment is to control the disease. The drugs approved for use in this setting are Pembrolizumab and Nivolumab. They are given as intravenous infusion every 2-3 weeks depending on the drug used. These drugs tend to have lesser side effects than chemotherapy but are more expensive and can cause significant side effects in some patients.
Hypopharynx
The hypopharynx is a part of the throat that is behind the larynx. It forms the lower part of the pharynx (throat) and has the oropharynx above it and the oesophagus (gullet) below it.
Symptoms from cancers of the hypopharynx can be varied but commonly include difficulty swallowing, feeling of a lump in the throat, changes to voice, pain on swallowing, coughing up of blood, earache or a lump in the neck. For investigations and diagnosis, see section on investigations in head and neck cancers.
Treatment of Cancers of Hypopharynx
Radiotherapy and Chemoradiotherapy
Treatment of hypopharyngeal cancer is mainly with radiotherapy and chemotherapy. For very early cancers that are stage I and 2, radiotherapy alone is the treatment of choice. Cancers that are stages 3-4 are treated with chemoradiotherapy, where chemotherapy and radiotherapy are given together.
When radiotherapy alone or chemoradiotherapy are used, the primary area of disease in the hypopharynx as well as the lymph node regions in the neck are treated. The treatment is usually given over 6 ½-7 weeks and is given daily 5 days a week. When the chemoradiotherapy is used, chemotherapy drugs such as cisplatin or carboplatin are given either once weekly or once every 3 weeks.
Neoadjuvant or Induction Chemotherapy
In some patients with very advanced hypopharyngeal cancer, chemotherapy can be considered prior to start of chemoradiotherapy to reduce the amount of disease. This way of treatment is called as neoadjuvant chemotherapy.
Surgery
Surgery is usually not an option of treatment for hypopharyngeal cancer except in some circumstances where there is a small and early stage cancer. This is particularly used if the larynx can be preserved and the cancer can be removed completely.
Chemotherapy
In patients with very advanced nasopharyngeal cancer that has spread to other parts of the body from the head and neck region, are treated with either radiotherapy or chemotherapy alone. The chemotherapy drugs commonly used in such a setting include cisplatin, carboplatin, fluorouracil, paclitaxel and docetaxel. In this setting treatment is mainly aimed at control of disease.
When the cancer is advanced, chemotherapy is sometimes used as an initial treatment to be followed by chemoradiotherapy or surgery. This option is called as neoadjuvant chemotherapy.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors.
The nasopharynx is part of the throat that lies behind the nose. It connects to the nasal cavity in the front and the oropharynx below it. Cancers of the nasopharynx are rare in India and risk factors for developing such a cancer include infection with a virus called EBV, smoking and use of tobacco products and eating salt cured meat and fish.
Symptoms produced by nasopharyngeal cancer include deafness or reduced hearing in one or both ears, earache, sore throat that is not settling, cough, bleeding through the nose, blocked nose and change in voice.
For investigations and diagnosis, see section on investigations for head and neck cancer.
Treatment of Nasopharyngeal Cancer
Radiotherapy and Chemoradiotherapy
Treatment of nasopharyngeal cancer is mainly with radiotherapy and chemotherapy. For very early cancers that are stage I, radiotherapy alone is the treatment of choice. Cancers that are stages 2-4 are treated with chemoradiotherapy, where chemotherapy and radiotherapy are given together.
When radiotherapy alone or chemoradiotherapy are used, the primary area of disease in the nasopharynx as well as the lymph node regions in the neck are treated. The treatment is usually given over 6 ½-7 weeks and is given daily 5 days a week. When the chemoradiotherapy is used, chemotherapy drugs such as cisplatin or carboplatin are given either once weekly or once every 3 weeks.
Adjuvant chemotherapy
Following completion of chemoradiotherapy, chemotherapy alone is considered in patients who are fit to be able to have such treatment. This chemotherapy is given for up to 4 cycles. This type of treatment is called as adjuvant chemotherapy.
Neoadjuvant chemotherapy
In some patients with very advanced nasopharyngeal cancer, chemotherapy can be considered prior to start of chemoradiotherapy. This way of treatment is called as neoadjuvant chemotherapy.
Surgery
Surgery is usually not an option of treatment for nasopharyngeal cancer except in some circumstances when there is a recurrence of cancer soon after radiotherapy.
Chemotherapy
In patients with very advanced nasopharyngeal cancer that has spread to other parts of the body from the head and neck region, are treated with either radiotherapy or chemotherapy alone. The chemotherapy drugs commonly used in such a setting include cisplatin, carboplatin, fluorouracil, paclitaxel and docetaxel. In this setting treatment is mainly aimed at control rather than cure.
When the cancer is advanced, chemotherapy is sometimes used as an initial treatment to be followed by chemoradiotherapy or surgery. This option is called as neoadjuvant chemotherapy.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors.
Oral cancers include cancers of the Lip, Tongue, Floor of mouth, Inside of the cheek, Gums, area behind the last molar tooth, and roof of the mouth.
Oral cavity cancers are very common in India due to the practice of chewing tobacco products. They account for about 10% of all cancers diagnosed in India.
Symptoms
Common symptoms in oral cancer include the presence of an ulcer in the mouth that does not heal, thickness of the skin or an area in the mouth, bleeding from the mouth, pain, red or white patches in the mouth, loosening of the teeth, lump in the mouth or neck. These symptoms could be due to causes not related to cancer but should be reported to a doctor. A thorough examination and a biopsy of any suspicious areas is needed.
Staging
The cancers in this area can be divided into early cancers (stages 1 and 2) and advanced cancers (stages 3 and 4). Treatment largely depends on the location and the stage of cancer at the time of diagnosis. Other factors include the general fitness of the patient and the anticipated functional results after the treatment.
Treatment of Oral Cavity Cancers
Surgery
Surgical treatment is usually the preferred option for treatment of oral cancers particularly in early cancers. Surgery can give good functional outcomes such as speech and swallowing after the treatment. Surgery involves removal of the tumour along with an adequate margin around the tumour. It may involve removing structures such as muscle and bone along with the tumour.
Surgery in oral cancer can be done using standard techniques or using laser or robotic techniques.
Lymph node dissection
A lymph node dissection or removal of lymph nodes in the neck is done in most patients who have surgery for oral cancers. The lymph node surgery may be on one or both sides of the neck and is dependent on the type of oral cancer and its location.
Surgery for tongue cancers involves removal of a part of the tongue (partial glossectomy) or the entire tongue (total glossectomy). If a total glossectomy is done, reconstructive surgery is done to enable the function of the tongue. In some cancers, a part of the upper or lower jaw has to be removed to enable complete removal of the cancer. Sometimes, a few teeth may have to be removed. While these surgeries are done and in the healing period, alternative forms of feeding may be needed in the form of nasogastric tube placement or PEG (gastrostomy tube-where a tube is placed in the stomach).
If muscles or part of the bone is removed, then reconstruction is done to preserve function as much as possible.
Radiotherapy
Radiotherapy is used as a primary treatment to treat oral cancers in patients with early tumours who are not medically fit to have surgery or those who choose not to have surgery. It is also used as an adjuvant treatment in patients who have had surgical resection and the margins are close or there are some high-risk features in the tumour. Here treatment is given over 6-7 weeks daily for 5 days a week. Radiotherapy is good in controlling the cancer but can give side effects in the form of sore mouth and throat, difficulty swallowing and eating and a dry mouth. Long term side effects are those which persist for longer than a few weeks after completion of radiotherapy, such as difficulty opening mouth, difficulty with eating or a dry mouth are an issue in patients with oral cancer who have radiotherapy.
Chemoradiotherapy
Chemoradiotherapy involves giving chemotherapy and radiotherapy together in patients with advanced oral cancers. Here, the radiotherapy is given for 6-7 weeks duration, daily for 5 days a week and chemotherapy given either once weekly or once in three weeks. The chemotherapy and radiotherapy together work better and provide a better chance of tumour control in advanced cancer.
Chemoradiotherapy is used as a primary treatment in patients whose disease is too advanced to enable a surgical resection or in patients who do not wish or are not offered surgery due to poor functional outcome. It is also used as an adjuvant treatment in patients who had resection of an advanced oral cancer. The side effects of treatment are more than radiotherapy alone and include symptoms described in the above section.
Chemotherapy
In oral cancers that are very advanced where there is spread of disease into other parts of the body such as lungs, liver etc, chemotherapy alone is used to help control the cancer. The intention of such treatment is to control the cancer rather than to cure it. Chemotherapy can be given in different formats with different drugs, but common drugs used include Cisplatin, Carboplatin and Taxanes.
When the cancer is advanced, chemotherapy is sometimes used as an initial treatment to be followed by chemoradiotherapy or surgery. This option is called as neoadjuvant chemotherapy.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors.
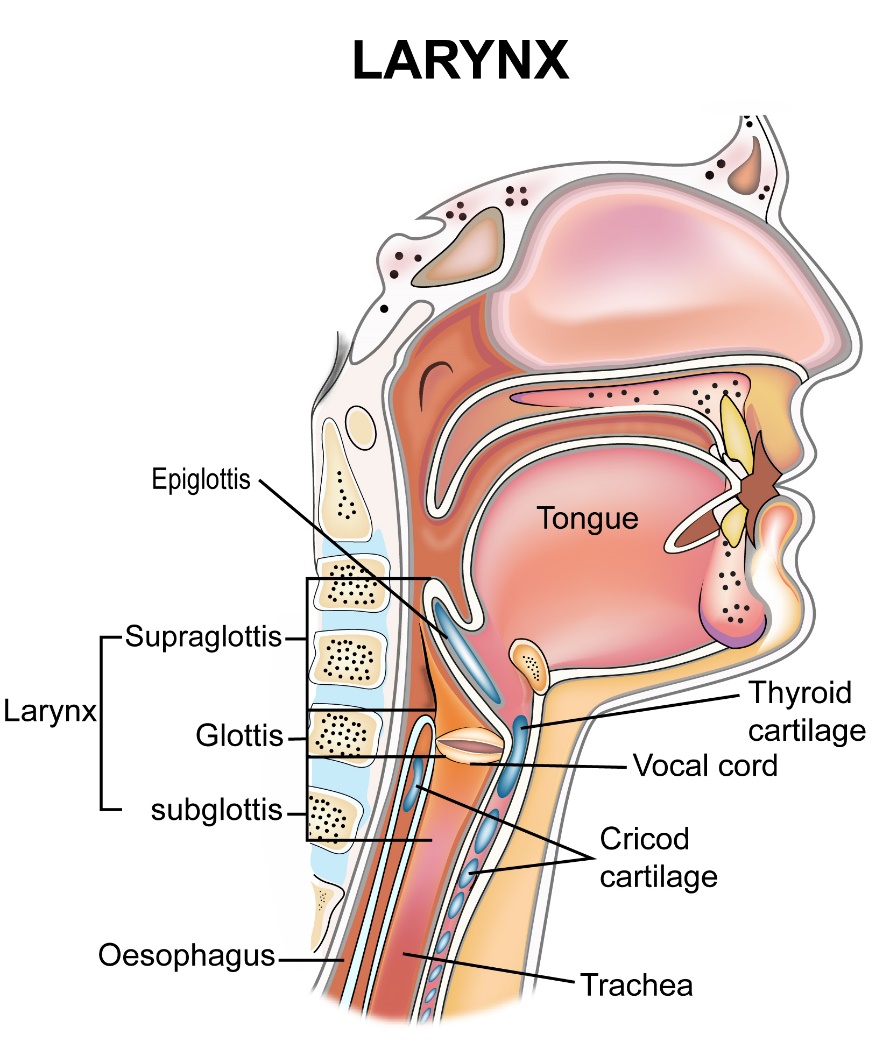
Laryngeal cancers are those that start in the larynx or voice box. The larynx is a tube-like structure present in the neck connecting the throat to the trachea or windpipe. The function of the larynx is to produce sound which is then converted into speech with the help of organs such as nose, mouth and tongue. These cancers can be divided into supraglottic-where the cancer starts above the vocal cords, glottic-where the cancer starts in the vocal cords and sub glottic-where the cancer starts in the larynx below the vocal cords. In Inida, larynx cancers account for 2.5% of all cancers.
Symptoms of larynx cancers include change or hoarseness of voice, feeling of a lump in the throat or neck, difficulty breathing or swallowing, pain in the neck, earache, persistent sore throat. The above symptoms occur due to other causes also including benign lumps in the larynx and should be looked at by a doctor if the symptoms persist or increase.
Tests used to look for larynx cancer include indirect laryngoscopy-where the doctor uses a small mirror to look into the throat, direct laryngoscopy-where a laryngoscope is used to look directly into the larynx and flexible nasendoscopy which is a thin tube with a camera attached at the end. Other tests include scan. For details look at investigations in head and neck cancer section.
Treatment of Laryngeal Cancers
The treatment for these cancers depends on the location of the tumour and the stage of the cancer at the time of diagnosis.
Treatment options include surgery, radiotherapy, chemoradiotherapy or a combination of these options. Apart from the stage of the cancer, preservation of function of the larynx is also an important aspect to take into account when deciding on the type of treatment option to take. In some instances, a choice of either radiotherapy or surgery is not available due to the nature and spread of the cancer to surrounding structures. In such instances, either of these treatment options is suggested.
Radiotherapy
Radiotherapy alone is an option of treatment for early stage cancers of the larynx. For cancers of the larynx that are advanced, chemoradiotherapy which is a combination of chemotherapy and radiotherapy is used. As compared to surgery, using radiotherapy or chemoradiotherapy helps in preserving the function of the larynx.
Surgery
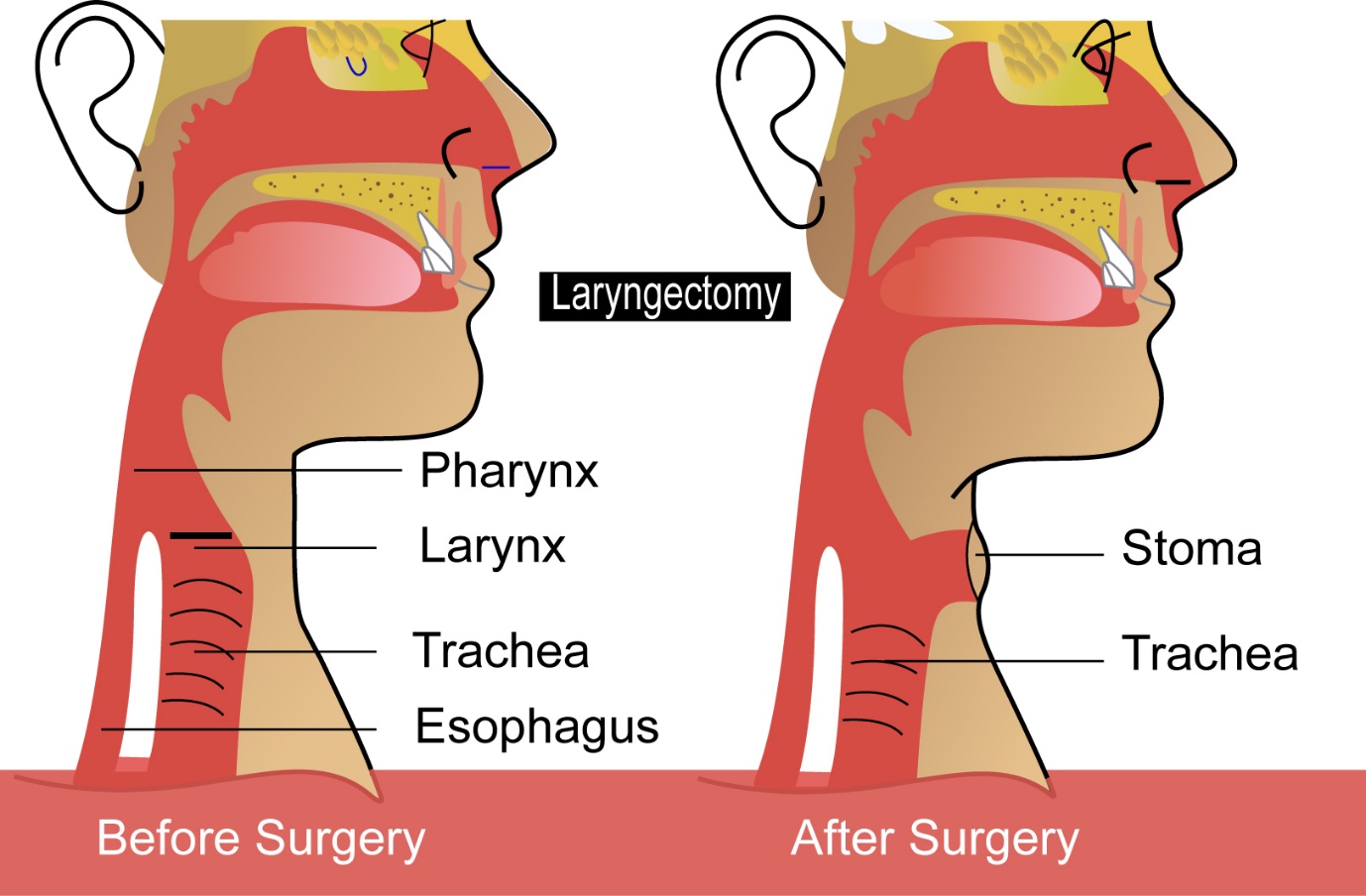
In early stage laryngeal cancers, surgical removal of the cancer is an option. Newer techniques such as transoral laser resection are now available which have limited side effects and good preservation of function. In advanced stage larynx cancer, surgical removal of the larynx is done along with removal of the lymph nodes in the area. Total removal of the larynx called total laryngectomy is sometimes needed to get rid of all the cancer. When this is done, a stoma(opening) is made at the bottom of the neck and the trachea or windpipe is attached to the stoma. The patient will breathe in and out through the stoma. The patient will not be able to speak once the larynx is removed and other methods are employed to allow the patient to communicate.
Voice Restoration after surgery
For patients who have a laryngectomy, which involves removal of the larynx, speech cannot be produced naturally. After surgery, other options or tools are available which help the patient to communicate. These options are listed below.
Prosthetic valve
A prosthetic valve helps in diversion of air from the stoma into the oesophagus through the valve.
As a result of air passing through, the valve vibrates and produces a sound. The sound can be articulated to produce speech. At the time of laryngectomy, a communication is made between the trachea and oesophagus in which the valve is placed. When the patient wants to communicate, he or she places their finger on the opening of the stoma to divert the air through the valve. The patient needs help and training to enable themselves to use this valve to make speech.
Electrolarynx
An electrolarynx is an electronic aid that produces vibrations. This aid is placed on the neck when the patient wishes to speak. The vibrations that are produced will help the patient to make sounds which can be articulated into speech. Help and training is needed for the patient to understand the technique and get used to its use.
Oesophageal speech
This is a technique where air is taken into the oesophagus and as the area moves back into the mouth, is able to make a sound that can be articulated to speech.
Chemotherapy
In larynx cancers that are very advanced, where there is spread of disease into other parts of the body such as lungs, liver etc, chemotherapy alone is used to help control the cancer. The intention of such treatment is to control the cancer rather than to cure it. Chemotherapy can be given in different formats with different drugs, but common drugs used include Cisplatin, Carboplatin and Taxanes.
When the cancer is advanced, chemotherapy is sometimes used as an intial treatment to be followed by chemoradiotherapy or surgery. This option is called as neoadjuvant chemotherapy.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors.
The oropharynx is the part of the throat that lies between the nasopharynx and hypopharynx. Oropharyngeal cancers involve tumours starting in the tonsil, tongue base and soft palate. The tonsils are present on either side of the throat. The tongue base is at the back of the tongue and the soft palate is the soft movable structure on the roof of the mouth.
Symptoms produced by cancers in the oropharynx include earache, swelling or lump in the throat or the neck, persistent sore throat, difficulty swallowing, bleeding from the mouth or nose, bad breath, speech and voice changes.
If suspected, examination and investigations will help in making a diagnosis of this cancer. See section on investigations in head and neck cancer for more details.
Treatment of Oropharyngeal Cancers
Oropharyngeal cancers can be treated with surgery or radiotherapy. The treatment choice depends on the location and stage of the cancer.
Surgery
Surgery is used as a treatment option in all types of oropharyngeal cancers, particularly early cancers. The surgery can be done by the open method, where an incision is made in the skin around the area of the mouth or neck and the cancer removed through that. Newer surgical techniques such as transoral surgery or transoral robotic surgery (TORS) or transoral laser microsurgery (TLM) use techniques that involve removal of the cancer through the mouth, thus avoiding an incision through the skin. These newer techniques are used to treat smaller cancers and cause less side effects as compared to the open method.
For certain cancers, parts of the upper or lower jaw, tongue, palate or other structures may have to be removed to complete the surgery. In such situations, reconstructive surgery is done to preserve function such as speech or swallowing.
Lymph node dissection
A lymph node dissection or removal of lymph nodes in the neck is done in most patients who have surgery for oropharyngeal cancers. This is done through a separate incision in the neck or through the same incision that is used to remove the primary cancer. Lymph node dissection is done even in patients where there is no evidence of enlargement of the lymph nodes. This is because, the risk of presence of microscopic disease is more in patients with oropharyngeal cancer. The lymph node surgery may be on one or both sides of the neck and is dependent on the type of cancer and its location.
Radiotherapy
Radiotherapy or chemoradiotherapy is a common option of treatment for oropharyngeal cancers.
The radiotherapy alone is used in patients after surgery when the risk of recurrence of cancer is felt to be high due to various factors seen at the time of surgery. Radiotherapy alone is also used as a main treatment in patients who are not fit to have chemoradiotherapy or in patients who have early stage disease.
Chemoradiotherapy involves use of chemotherapy and radiotherapy at the same time. This treatment is more intensive than radiotherapy alone and is used either after surgery or as the main treatment for advanced oropharyngeal cancer. Chemoradiotherapy-like radiotherapy is used either after surgery or as the main treatment. The chemotherapy drugs commonly used in this setting are cisplatin, carboplatin or taxanes. Cetuximab is a targeted agent which acts against EGFR receptor and can be used combined with radiotherapy instead of chemotherapy in some patients.
Chemotherapy
In oropharyngeal cancers that are very advanced where there is spread of disease into other parts of the body such as lungs, liver etc, chemotherapy alone is used to help control the cancer. The intention of such treatment is to control the cancer. Chemotherapy can be given in different formats with different drugs, but common drugs used include Cisplatin, Carboplatin and Taxanes.
When the cancer is advanced, chemotherapy is sometimes used as an initial treatment to be followed by chemoradiotherapy or surgery. This option is called as neoadjuvant chemotherapy.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors. For more details, see section on treatment of head and neck cancers.
Salivary glands are present in the head and neck region. Their function is to produce saliva which keeps the mouth wet and moist and helps in eating and swallowing food. Salivary glands can be major glands and minor salivary glands. The major glands include the Parotid gland, the Submandibular gland and the Sublingual gland. One of each are present on each side of the head. There are a number of minor salivary glands present around the mouth which are very small and also produce saliva.
Salivary gland tumours are of different types, some of them being benign tumours and others being malignant ones.
Common tumours that can form in the salivary glands include
Pleomorphic adenoma
Warthin’s tumour
Mucoepidermoid Carcinoma
Adenoid cystic Carcinoma
The symptoms produced by these salivary gland tumours include lump or swelling on the face or neck, pain on eating, difficulty chewing or pain on chewing, weakness or numbness on the face.
Treatment of Salivary Gland Tumours
The treatment strategies will differ depending on the type of tumour. They will also depend on the stage and location of the tumour.
Surgery
Surgery is one of the main options of treatment of salivary gland tumours and cancers. Surgery aims to remove the tumour as well as the salivary gland that contains the tumour. If the tumour is extensive and involves other structures around the salivary gland, they are also removed along with the tumour.
Tumours of the parotid gland are treated with a parotidectomy, which means removal of the parotid gland. In benign tumours, a superficial parotidectomy is done where only a part of the parotid gland is removed. In malignant tumours, the whole parotid gland may need to be removed. The parotid gland contains the facial nerve, which supplies function to the muscles of the face and care is taken to avoid damage to this nerve at surgery. In malignant tumours, when the nerve is already affected and is non-functional, the nerve is removed along with the gland. Other structures around the parotid gland that are involved by the tumour are also removed.
Tumours of other salivary glands such as submandibular and sublingual gland are removed with surgery. Removal of the lymph nodes in the neck is done at the same time the cancer is removed. Lymph node surgery is done when there is a risk of cancer spreading into the lymph nodes.
Radiotherapy
Radiotherapy is used in salivary gland tumours and cancers usually after surgery. The reasons to use radiotherapy after surgery include close or positive margins of resection which means that the cancer cells were too close to the margin of surgery. Here radiotherapy is given on a daily basis, 5 days a week for 5-7 weeks depending on the type of tumour. Radiotherapy is also used for tumours that have recurred after a surgery was done previously or in situations when the disease is too extensive for surgery to be done or where there is a higher risk of recurrence of tumour even after complete removal as in the case of some malignant salivary gland tumours.
Chemotherapy
Chemotherapy is used for salivary gland cancers that have spread to different parts of the body. Here chemotherapy is used to control the cancer and any symptoms that the cancer produces.
Immunotherapy
Immunotherapy is used as a treatment in advanced stage 4 or recurrent head and neck cancer. Drugs used in Immunotherapy include Nivolumab and Pembrolizumab which are classed as PD-1 inhibitors.
