

Kidneys are organs present in the back of the abdomen. There are two kidneys, right and left, present on either side of the spine. The kidneys are connected to the bladder through the ureters and along with these forms the excretory system of the body. The blood enters the kidney through the renal artery and comes out through the renal vein. At the top of each kidney is a gland called adrenal gland which produces hormones.
The function of the kidneys is to filter the blood that passes into it and remove waste products.
The kidneys help maintain the balance of fluids and salts in the body and also helps maintain the blood pressure.


Kidney cancer is one where the cancer originates in the cells of the kidneys. There are different types of renal cancers, but the most common one of all which makes up about 85% is called as clear cell renal cell carcinoma. The uncommon ones are called as papillary, chromophobe, oncocytic or collecting duct carcinoma. According to Globocan 2018 data, there were 15,454 cancers in 2018 making up 1.3% of all cancers.
Kidney cancer can occur due to a number of potential causes. The common ones are listed below. Kidney cancer usually affects one kidney. It is very unusual for both kidneys to have cancer at the same time.
Smoking
Smoking is a risk factor for renal cancer. The probability of getting renal cancer is increased in smokers as compared to non-smokers by about a third.
Obesity
Being obese or overweight increases the risk of getting kidney cancer. Studies have shown that about 20% of kidney cancers can be related to obesity.
Age
The risk of getting kidney cancer increases with age. It is generally rare in patients under 50 years of age and commoner in those aged above 70 years.
Kidney disease
People with long term kidney disease have a higher risk of developing kidney cancer. This risk is increased in those having dialysis.
Family History
The risk of getting kidney cancer increases if someone in the close family had it like a brother, sister, mother or father.
Genetic causes
People with inherited genetic conditions such as Von-Hippel Lindau syndrome, tuberous sclerosis or BHD syndrome have a higher risk of getting kidney cancer compared to the normal population. The cancers that develop in these conditions happen at a younger age and can be multiple and involve both kidneys.
Kidney cancer may not produce any symptoms when it is small and may be found incidentally after tests for another reason. The symptoms that can be produced from kidney cancer include
Blood in the Urine
Having blood in the urine is a common symptom associated with kidney cancer. The bleeding can be on and off. Sometimes bleeding may not be visible to the eye and may only be found on microscopic tests.
It is important to note, that blood in the urine can be caused by a lot of other conditions such as infections, kidney or bladder stones etc.
Pain
Presence of a dull aching pain in the loin (area between back and upper abdomen) can be a symptom due to kidney cancer.
Fever and night sweats
Having fever along with tiredness and sweating at night is a symptom of renal cancer. It is also a common symptom for infections.
Lump or Mass
Presence of a lump or a mass on the side of the abdomen can be a sign of renal cancer.
Other symptoms
Other symptoms such as reduced appetite, weight loss, swelling in the legs or scrotum, anaemia and feeling unwell can all be symptoms of kidney cancer.
As part of investigations into the diagnosis of cancer, all patients have an examination done by the doctor along with a set of blood tests. Common tests include complete blood picture or full blood count, electrolytes, creatinine, liver function tests and any specific blood tests for that particular type of cancer. Other tests include,
Ultrasound scan
An ultrasound scan uses sound waves to look for abnormalities. In kidney cancer, an ultrasound scan helps detect lumps or masses present within the kidneys. The ultrasound scan may not always be able to tell whether the kidney mass is cancer or not as there are other noncancerous lumps like kidney cysts which are also very common. Other tests may also be needed.
CT Scan
A CT scan of the abdomen or a CT Urogram is done when investigating for kidney cancer. The CT scan can give detailed images of the abnormal area which will help in identifying the nature of the abnormal mass. The scan also helps in staging the disease after a diagnosis is made. A CT Urogram is a special type of CT scan which helps to look specifically for abnormalities in the renal tract. This involves the kidneys, ureters and bladder.
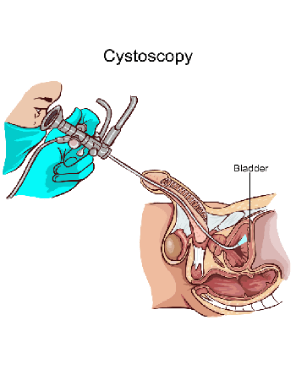
Cystoscopy
In patients presenting with blood in the urine, cystoscopy it is a common test performed to look for a cause for this bleeding. A cystoscopy involves placing a thin tube through the penis to have a look in the bladder. The tube has a light source and a camera attached to it which enables the doctor to look inside the bladder.
MRI scan
An MRI scan uses strong electromagnetic waves to look at the inside of the body. This scan is sometimes used to identify the nature, size and spread of the mass present on the kidney. MRI scan is used to tell the difference between kidney cancer and a non-cancerous lump called an angiomyolipoma.
Bone scan
An isotope bone scan is used for staging of kidney cancer. The bone scan helps to identify the presence or absence of kidney cancer in the bones.
Kidney biopsy
A biopsy is a test where a sample of tissue is taken with a needle and looked under the microscope to make a diagnosis. In kidney cancer, particularly in advanced kidney cancer, a biopsy is done to confirm the diagnosis prior to the start of treatment. In early kidney cancer, a biopsy is not usually done prior to removal of cancer.
PET-CT Scan
A PET/CT scan is not routinely recommended for the staging of kidney cancer at the time of diagnosis as it is not very accurate in this setting.
The stage of a cancer is a term used to describe the size and location of the cancer in the body. Knowing the stage of the cancer helps the doctors to decide on the most appropriate treatment. Kidney cancer is staged based on the TNM staging system or the number system.
Staging with either system is based on the size and extent of the tumour in the kidney, the spread of the cancer in the kidney and into the lymph nodes or surrounding blood vessels and spread of cancer into other parts of the body.
TNM stands for tumour, node and metastases. T stands for tumour and N stands for nodes and spread of cancer into lymph nodes around the kidney. M stands for metastases and spread of cancer to distant areas in the body.
TNM Staging
T Stage
| T1 | Here the cancer is confined to the kidney only and is 7cm or smaller In size |
| T2 | The cancer is confined or limited to the kidney and is more than 7cm In size |
| T3 | The cancer extends to areas outside the kidneys or into blood vessels (renal vein, fat, inferior vena cava) |
| T4 | The cancer spreads to areas further away from the kidney or to adrenal gland |
N Stage
| N0 | There is no involvement of lymph nodes by the cancer |
| N1 | The cancer has spread into the surrounding lymph nodes |
M Stage
| M0 | There is no spread of cancer into distant parts of the body |
| M1 | There is spread of cancer into distant parts of the body |
Number Staging
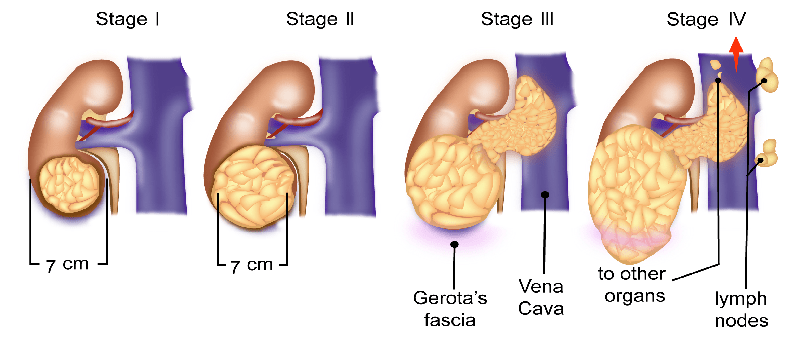
| Stage 1 | The cancer is in the kidney and is 7cm or smaller in size |
| Stage 2 | The cancer is in the kidney only and is larger than 7cm in size |
| Stage 3 | The cancer has spread to the outside of the kidney into the veins or renal fat or into nearby lymph nodes. |
| Stage 4 | The cancer has spread into the outside layer of the kidney or into the adrenal gland or into distant parts of the body. |
Treatment of the kidney cancer is largely dependent on the stage of cancer at diagnosis. The following options are used in the treatment of kidney cancer.
Surgery
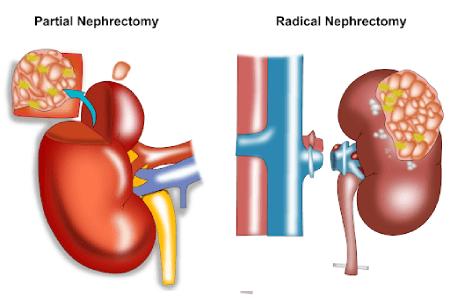
In cancer that is present only in and the around the kidney and has been taken out completely, further treatment is not needed. However, in patients with disease present at the margins of surgery or has spread to other parts of the body, further treatment is advised after the nephrectomy. Nephrectomy can be done in many ways. The common way to do this operation is an open nephrectomy where a large cut is made in the loin and the cancer is removed through that. The other option is laparoscopic surgery. The third option is a robotic nephrectomy where laparoscopic surgery is done with the help of a robot. Laparoscopic and robotic surgeries are better than open surgery in experienced hands and have faster recovery times but are not possible in all situations.
Surgery for Stage 4 Cancer
Surgical removal is mainly for the removal of kidney and neighbouring structures as described above but the removal of kidney cancer that has spread to other parts of the body is occasionally done when such surgery is capable of removal of all metastatic disease. For example, when there is a spread of cancer into only one or two parts of the lungs, liver or brain, surgery and removal of those areas are done with good outcomes. In patients with advanced or metastatic cancer that cannot be cured with surgery alone, a debulking surgery is done which is described below.
Treatment of Advanced or Metastatic Renal Cancer
Most patients diagnosed to have advanced or metastatic renal cancer who cannot be cured with surgery alone are treated with surgery plus systemic therapy in the form of Biological therapy or Immunotherapy or a combination of both. Prior to having such therapy, most patients undergo debulking surgery where the primary tumour or cancer present in the kidney is removed and systemic treatment is started after that. In some situations where the disease is extensive or the patient is not fit enough to have surgery, systemic therapy is started first followed by surgery later. This surgery is different from the surgery described above where this is to reduce the bulk of the disease rather than to cure it.
Risk stratification in Advanced or metastatic Renal cancer
All patients with advanced and metastatic renal stratification are placed into three groups based on certain characteristics of the patient and cancer. These three groups are a good risk, intermediate risk and poor risk. The systemic treatment that is planned for the patient is dependent on which group the patient falls into. Options of treatment include either biological therapy alone, Immunotherapy alone or a combination of both, particularly in intermediate and poor-risk groups. The benefits and risks of these treatments will be discussed by the oncologist before an option is selected.
Biological Treatment
Biological treatment or targeted treatment involves the use of drugs that target specific sites either on the cancer cells or on mechanisms that enable cancer to grow. A number of these biological drugs are available for the treatment of kidney cancer.
Biological treatment is used in patients with advanced kidney cancer where cancer cannot be removed by surgery or where cancer had spread to different parts of the body (metastatic).
These drugs are given as tablets or into the vein. They help reduce cancer, control symptoms and prolong life. Drugs commonly used are Sunitinib, Pazopanib, Cabozantinib, Sorafenib, Axitinib, Bevacizumab, mTOR inhibitors such as Temsirolimus and Everolimus.
The common side effects of these targeted therapies include tiredness, diarrhoea, skin changes, sore mouth, low blood counts and risk of infection, muscle aches, changes in the function of the thyroid gland and blood pressure. Along with these, each drug has its own list of specific side effects.
Immunotherapy
Drugs that have an effect on the immune system are used in renal cancer. These drugs boost the immune system to fight against cancer. The commonly used drugs are cytokine drugs such as Interferon alfa and Interleukin. Checkpoint Inhibitors such as Nivolumab and anti-CTLA antibody such as Ipilimumab. Nivolumab and Ipilimumab or a combination of both are drugs used in the treatment. See section on Immunotherapy in FAQ’s for more details such as side effects etc.
Chemotherapy
Chemotherapy is not an established form of treatment for renal carcinoma.
Radiotherapy
Radiotherapy is sometimes used in the treatment of renal carcinoma. It is used at a time when surgery has been done and the margins at the end of resection specimen are positive, indicating the probable presence of disease at the tumour site. Radiotherapy is also used to treat symptoms such as pain, bleeding etc that are being caused by cancer that has spread to different parts of the body.
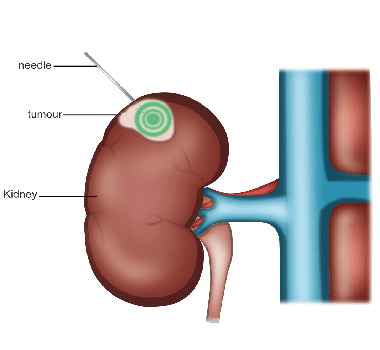
Radiofrequency Ablation (RFA)
It is also sometimes used in patients with advanced cancer, where the mass in the kidney is causing symptoms and cannot be removed by surgery. It can be used to treat small areas of cancers that have spread to the lungs or liver.
The procedure involves introducing a needle or a probe into the tumour through the skin. Radiofrequency waves are then transmitted through the probe which generates heat and destroys the tumour. This procedure is done with a local or general anaesthetic.
Cryotherapy
This is another form of treatment used in settings similar to RFA. Here extreme cold is used to kill cancer. A probe is inserted into the tumour through the skin. The probe or needle that is inserted has liquid Nitrogen inside it which then freezes and destroys the tumour.
This type of treatment is used in patients who have small renal cancers in the kidneys and are not fit for surgery. The treatment may be curable and can be used again if the tumour recurs.
Tumour Embolisation
Tumour embolisation is a process where the blood vessel supplying blood to the cancer is embolised(blocked). This starves the tumour of blood and oxygen and the tumour cells die. Embolisation is achieved by injecting a chemical into the blood vessel which then stops the flow of blood in that vessel. In kidney cancer, this procedure is used when cancer sannot be removed by surgery due to various reasons. It can also be used prior to surgery in some situations particularly when a large tumour is present and is likely to bleed at the surgery.
