

Lymphoma is cancer of the lymphatic system. The lymphatic system consists of lymph nodes present all over the body, the lymph vessels that connect these lymph nodes with each other. Organs such as the spleen, thymus gland, bone marrow and tonsils are also part of the lymphatic system. Lymphocytes, which are white blood cells present in the blood and bone marrow are also part of the lymphatic system.
The function of the lymphatic system is to drain fluid from the organs and to protect the body from infections. When infection is present in a part of the body, the lymph nodes in that area try and stop the infection from spreading to other parts of the body. This can lead to enlargement of the lymph nodes as seen commonly.
There are two types of lymphoma. One is called as Hodgkin lymphoma and the other one is called as Non-Hodgkin Lymphoma.
Non-Hodgkin lymphomas make up about 80% of all lymphomas. They do not contain Reed Sternberg cells when seen under the microscope. These lymphomas can again be divided into a number of subtypes depending on their appearance when seen under the microscope. They are also classified into low grade, intermediate grade and high grade Non-Hodgkin lymphoma (NHL).
Non-Hodgkin lymphoma can be of many types. Based on the cell of origin, they can broadly be classified into
- T Cell Lymphomas
- B Cell lymphomas
They can also be classified based on how they appear when seen under the microscope.
The common varieties seen are-
- Diffuse large B cell Lymphoma
- Mantle cell lymphoma
- Burkitt cell lymphoma
- Follicular lymphoma
- Lymphoplasmacytic lymphoma
- Small lymphocytic lymphoma/Chronic lymphocytic lymphoma
- Marginal zone lymphoma
- NK and T cell lymphoma
According to Globocan data 2018, there were 28,110 new non-Hodgkin lymphoma cancers in India in 2018, making up 2.4% of all cancers.
Non-Hodgkin Lymphoma can produce a number of symptoms. In patients with early disease symptoms may be very minimal.
Swelling and Enlargement of Lymph nodes
A common symptom seen is enlargement of lymph glands in the body. This can be in the area of the neck, under the arm pit, groins or in other parts of the body such as in the chest or stomach. These swellings are usually painless but can occasionally cause pain. Lymph nodes can enlarge due to a number of reasons including infections and not always due to a lymphoma.
Other Symptoms
Other symptoms commonly associated with Non-Hodgkin lymphoma include fever, loss of weight, excessive sweating at night, excessive itching of the skin, cough, difficulty breathing or stomach pains.
Symptoms due to anaemia or symptoms such as easy bruising, bleeding or infections can happen if there is involvement of the bone marrow by the lymphoma.
A type of Non-Hodgkin lymphoma called Primary CNS lymphoma occurs in the brain or spinal cord and can produce symptoms such as headaches, fits, changes in eye sight, dizziness, unsteadiness etc. As lymphomas can occur at any area in the body, the symptoms can be very different from one patient to the other.
When a lymphoma is suspected, either a Hodgkin or a Non-Hodgkin lymphoma, the following investigations are usually done.
Biopsy
A biopsy of the enlarged lymph node is done to confirm the presence of a lymphoma. This is either a core biopsy (core of node) or an excision biopsy where the entire lymph node is removed. Another type of biopsy called FNAC is not done in this setting. Immunohistochemistry (IHC) markers are special tests done on the biopsy sample to identify the specific type of lymphoma. Sometimes, a number of IHC markers are tested to know the exact type of lymphoma and to determine the right treatment. If a lump or a mass is present separate to a lymph node, a biopsy of the lump is done. Genetic tests to look for changes in chromosomes may be done to confirm or exclude certain types of lymphomas.
CT scan or PET-CT scan
A CT scan or a PET-CT scan is an ideal test to look for the extent of spread of the lymphoma. The scan is used to help in the staging process of the condition and will give information as to where the cancer is present in the body. A PET-CT scan is better than a CT scan to diagnose and stage the lymphoma. These scans are also done in patients having chemotherapy for lymphoma, to see how well the cancer is responding to treatment.
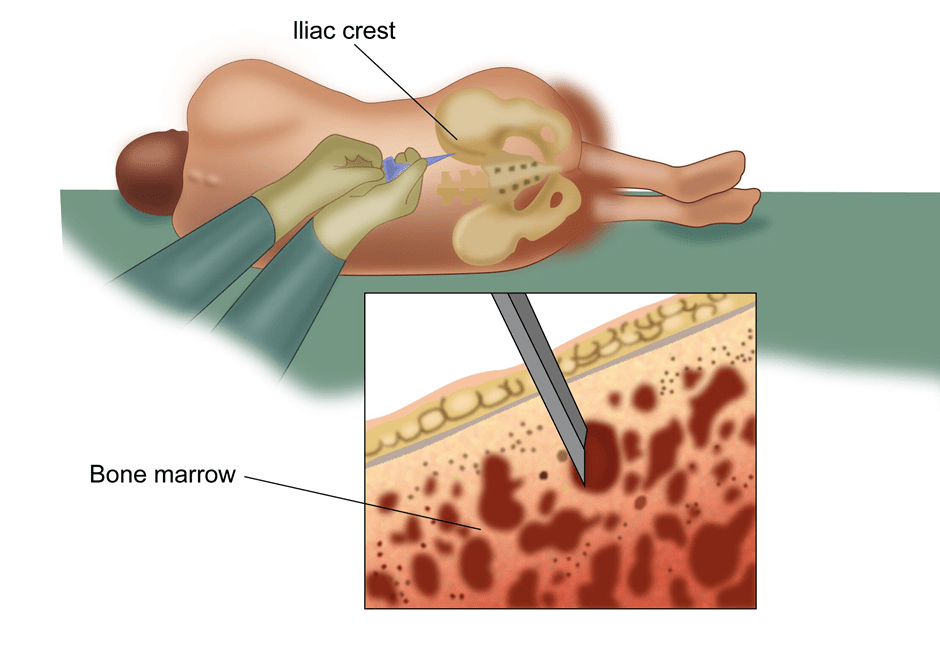
Bone Marrow Biopsy
A bone marrow biopsy involves taking a sample of cells from the marrow of the bone. This is an important test in lymphoma to look for spread of this cancer into the bone marrow. This biopsy is done under local anaesthesia. A bone marrow test may not be done in patients where a PET-CT scan does not show any disease in the marrow.
Blood Tests
A number of blood tests such as CBP, ESR, LDH, Liver function tests, Creatinine, Electrolytes and others are done routinely to assess the functions of various organs.
Other Tests
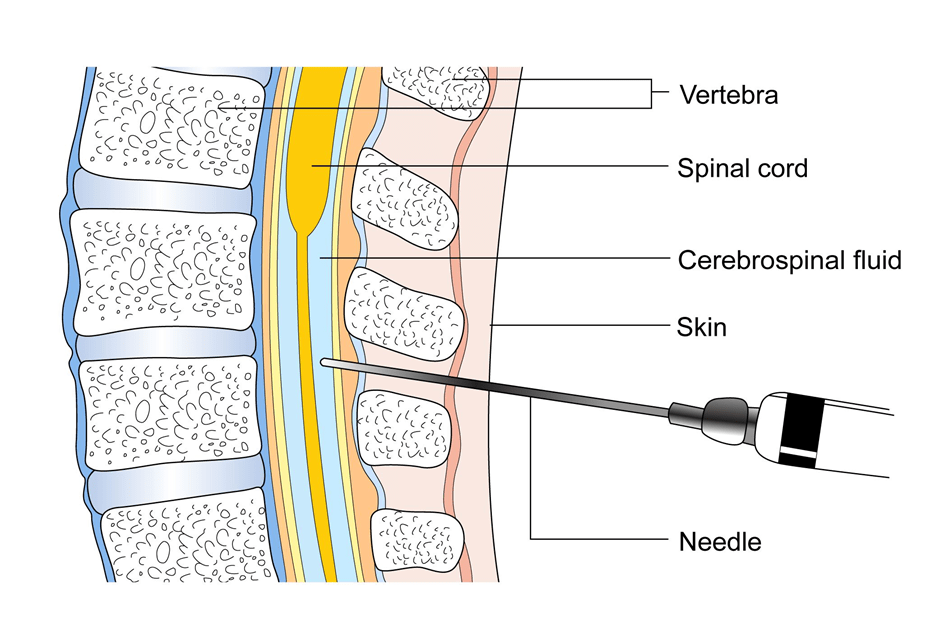
Other tests such as X rays, Ultrasound scan of the abdomen, MRI scans may also be used in some situations to gain more information about the disease. A lumbar puncture where a needle is placed in the spine to get a sample of fluid is done in some situations.
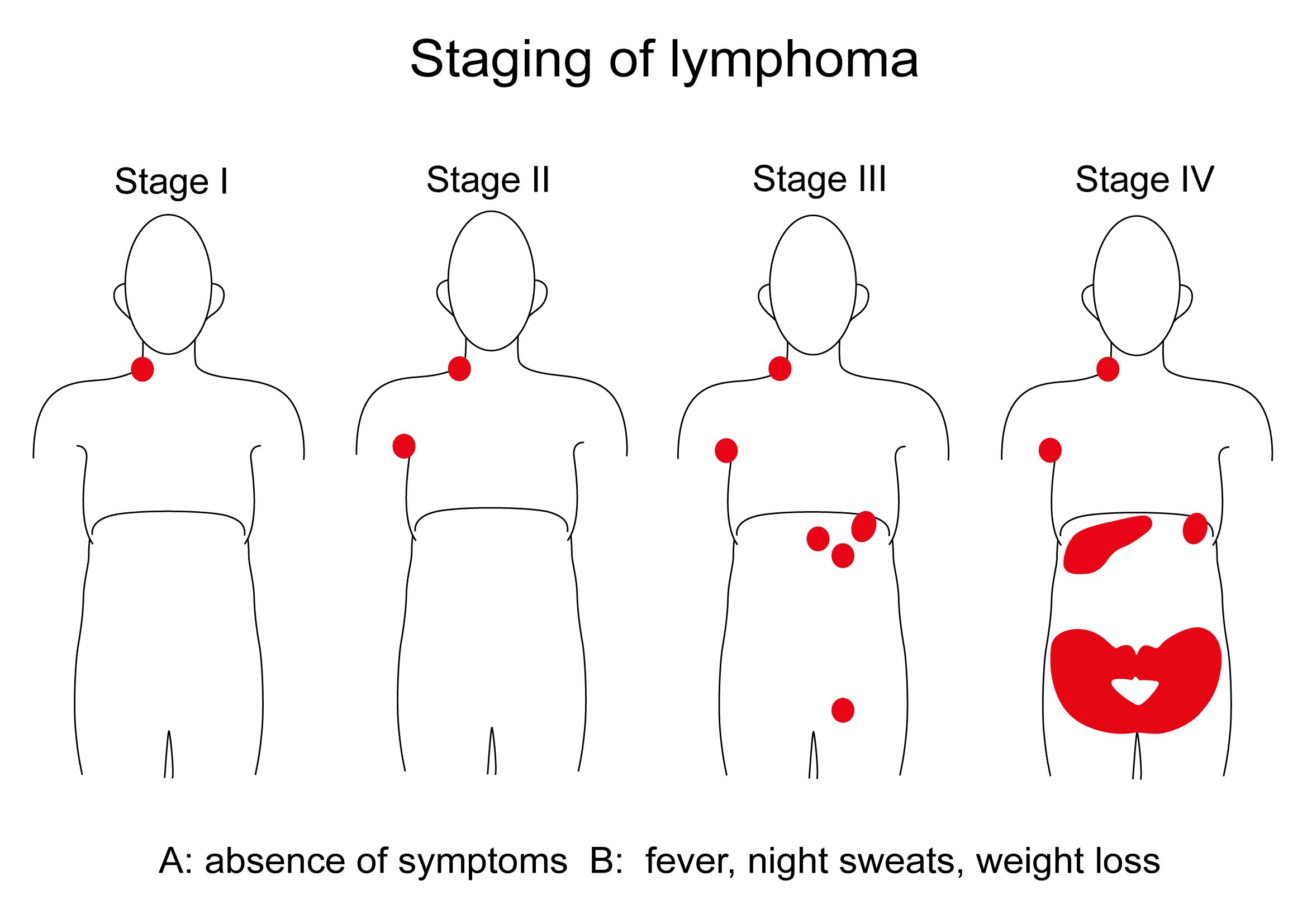
Stage I
In stage 1, there is Involvement of a single lymph node region (I) or of a single extra lymphatic organ or site (IE) without lymph node involvement. A single lymph node region can include one node or a group of adjacent nodes.
Stage II
In stage 2, there is involvement of two or more lymph node regions on the same side of the diaphragm (muscle separating chest and abdomen) alone (II) or with involvement of limited, contiguous organ or tissue that is not a lymph node (IIE).
Stage III
In stage 3, there is involvement of lymph node regions or lymphoid structures on both sides of the diaphragm.
Stage IV
In stage 4, there is additional non-contiguous extra lymphatic involvement, with or without associated lymphatic involvement.
All lymphomas are sub classified to indicate the absence (A) or presence (B) of one or more of the following three systemic symptoms: unexplained fevers to more than 101°F, drenching night sweats, or unexplained weight loss exceeding 10 percent of body weight during the six months prior to diagnosis. Fatigue, itching, and alcohol-induced pain are not considered B symptoms but should be noted.
Treatment of Non-Hodgkin Lymphoma depends on the type of lymphoma and whether it is a low grade or a high-grade Lymphoma. Treatment strategies also depend on the stage of Lymphoma at the time of diagnosis.
Treatment options for Non-Hodgkin Lymphoma include Chemotherapy, Radiotherapy, Biological therapy, Stem cell and Bone marrow transplants. In some situations, a wait and watch approach is also a strategy.
Treatment of Low-Grade Non-Hodgkin Lymphoma
Low grade lymphomas are usually slow growing compared to high grade lymphomas. Follicular Lymphoma is one of the commonest type of low grade Non-Hodgkin Lymphoma.
Early stage 1 and 2 low grade Lymphomas
These lymphomas are treated with radiotherapy. This treatment usually is for about 2 to 3 weeks duration.
Stage 3 and 4(advanced) follicular lymphomas
These lymphomas are varied, and treatment options include
Chemotherapy with a combination of drugs, for example R-CVP which includes drugs such as Cyclofosfamide, Vincristine, Prednisolone and Rituximab. Chemotherapy is given up to 6 cycles with each cycle lasting 21 days. A scan is done after 3 cycles to assess response to treatment. Blood tests are done before every cycle of chemotherapy.
Chemotherapy with a single drug or two drugs. Common drugs used here include Bendamustine, Lenalidomide.
Biological therapy includes drugs such as Rituximab and Obinutuzumab. These drugs are antibodies to CD20 lymphocyte and are used either alone or in combination with chemotherapy described above in low grade lymphoma.
Common side effects of chemotherapy include nausea and vomiting, hair loss, tiredness, soreness in the mouth, loss of taste, low counts of cells in the blood, risk of infection and bleeding. Most of the chemotherapy used in low grade lymphoma is tolerated well
A wait and watch approach-where no treatment is given and patient is monitored closely. Treatment is given when there is significant increase of cancer.
Following completion of initial treatment, maintenance treatment with Rituximab is an option. If there is a recurrence of the lymphoma after initial treatment, then another course of chemotherapy is used to control the disease. Usually advanced follicular lymphoma is very much controllable with treatment but not curable. In some patients where is disease still present after end of chemotherapy, radiotherapy may be given.
High Dose chemotherapy and stem cell or bone marrow transplant
Patients whose disease has relapsed or does not improve with chemotherapy may be suitable for high dose chemotherapy and stem cell or bone marrow transplant. This is not a common treatment but can be used in some situations. See section on stem cell and bone marrow transplant in lymphomas for more details.
Maintenance Treatment
Patients who have a good response to chemotherapy plus Rituximab treatment for low grade lymphoma can continue maintenance Rituximab once every two months for up to two years.
High grade Non-Hodgkin lymphomas are more fast growing and are usually treated with chemotherapy, radiotherapy and stem cell and bone marrow transplants.
Treatment of Early stage High grade Non-Hodgkin Lymphoma
Treatment of this type of lymphoma involves chemotherapy in the first instance followed by Radiotherapy to the area of body where the lymphoma was present. In a common form of high-grade lymphoma called diffuse large B Cell lymphoma, the common chemotherapy regimen used is called as CHOP-R, with each letter standing for the names of the drugs used.
- C-Cyclofosfamide
- H-Doxorubicin
- O-Oncovin (Vincristine)
- P-Prednisolone
- R-Rituximab
This type of chemotherapy is usually given once every 21 days and is given 4 times. This will be followed by radiotherapy which could last up to three to four weeks. Radiotherapy is given to the area of the body where disease was present prior to start of chemotherapy.
For other types of high-grade lymphomas, chemotherapy selected may be different and the duration of treatment may be longer, and radiotherapy may not be used in all circumstances.
Treatment of stage 3 and 4 (advanced) high grade Non-Hodgkin lymphoma
For advanced stage high grade lymphomas, the mainstay of treatment is chemotherapy. CHOP-R is used as chemotherapy for advanced stage diffuse large B cell lymphomas. Chemotherapy is given once every 21 days for up to 6 times. Other chemotherapy options may be selected for other types of high-grade lymphomas.
Radiotherapy is used sometimes after chemotherapy particularly in patients where there was large amount of disease at the time of diagnosis (bulk disease) or there is disease remaining after completion of chemotherapy.
Stem Cell or Bone marrow transplant for Non-Hodgkin Lymphoma
This is a treatment option for patients whose disease come back after initial treatment or does not respond very well to treatment. Here high dose chemotherapy is given first to control the disease followed by stem cell or bone marrow transplant. For more details of this treatment, see section on stem cell and bone marrow transplant in non-Hodgkin lymphomas.
Other Chemotherapy
Patients who have recurrence of disease after initial treatment and not suitable for stem cell or bone marrow transplant are treated with more chemotherapy. The drugs used will be different to the ones used before unless there is a long gap between the two treatments. The chemotherapy regimens used here include Gemcitabine, Lenalidomide, Bendamustine, Rituximab, Vinorelbine.
Radiotherapy Alone
Radiotherapy alone can be used as a treatment to control disease when it is causing any local symptoms such as pain. This type of treatment is usually only to control the cancer in that area.
Apart from the high and low grade lymphomas which are mentioned in other sections, some rarer forms of lymphomas are treated differently and these are briefly listed below.
Cutaneous T Cell Lymphoma
This is a type of T cell lymphoma where the disease is mainly present on the skin. A number of subtypes of cutaneous T cell lymphomas are present. The patient complains of a rash on the skin that is growing slowly over a period of weeks or months and not settling down.The diagnosis of this type of lymphoma is confirmed on a biopsy of the skin that is affected. A scan of the body such as a CT scan is done to look for presence of disease in other organs of the body. This helps in staging of the disease.
Treatment options in general for cutaneous lymphomas include application of topical chemotherapy agents to the skin areas, local radiotherapy to the skin, use of phototherapy such as PUVA and UVB rays. For disease that is extensive or has spread to other organs too, then standard chemotherapy, biological therapy or total skin electron radiotherapy are used as treatments.
Burkitt’s Lymphoma
This is a type of high-grade B cell lymphoma that happens due to an expression of an abnormal gene. This type of lymphoma is common in children and there can be different forms such as endemic, sporadic and immunodeficiency. Patients present with a rapidly growing tumour masses on the face or other parts of the body. They can be very unwell with the condition. Biopsy, IHC and genetic testing is done to confirm the diagnosis of this type of lymphoma. Treatment is dependent on the stage of the disease at diagnosis and usually involves chemotherapy with a combination of drugs. The chemotherapy lasts from a few weeks to many months depending on the extent of disease.
MALT or Marginal Zone Lymphoma
This is a slow growing type of B cell non-Hodgkin lymphoma which can occur in the lymph nodes, spleen or other organs such as stomach, lung, salivary glands, intestine or eyes.
In patients with MALT lymphoma of the stomach, the disease is said to occur due to infection of the stomach with an organism called H. Pylori which also causes stomach ulcers. In such a situation treatment is aimed at eradicating the organism. Radiotherapy is also used to control the disease. Chemotherapy or biological therapy with Rituximab is also an option in some patients.
In MALT lymphomas at other sites, radiotherapy is used for stages 1 and 2 and chemotherapy, radiotherapy or biological therapy is used as treatment in other stages.
Mantle Cell Lymphoma
This is an uncommon variant of B cell lymphoma with which patients complain of enlarged lymph nodes and on investigations, there may be involvement of other organs live spleen and bone marrow. Treatment is usually in the form of chemotherapy and Rituximab which is an antibody against CD20 lymphocyte. The chemotherapy drugs used include Bendamustine, CVP, CHOP among others. Autologous transplant with stem cells is considered in young and fit patients after initial chemotherapy.
Primary CNS Lymphoma is a type of Lymphoma that starts in the brain or other structures such as eyes, spinal cord or meninges of the brain. Its features, behaviour and treatment are different to that of lymphomas that begin in other parts of the body.
Symptoms of Primary CNS Lymphoma
This type of lymphoma produces symptoms related to the brain. Common symptoms include headaches, fits, confusion, reduced memory, change in personality, reduced eye sight, vomiting and weakness of different parts of the body.
Investigations for Primary CNS Lymphoma
When this type of cancer is suspected or the patient presents with above symptoms, the following tests are done.
MRI Scan
An MRI scan of the brain is commonly done to look for abnormalities in the brain when a patient presents with above symptoms. A CNS lymphoma is one of the possible causes for these symptoms and is seen on the MRI scan.
CT Scan
In places where an MRI scan is unavailable, a CT scan is used to look for abnormalities in the brain.
CSF Analysis
CSF or cerebrospinal fluid is the fluid that is present in the ventricles of the brain and in the spinal cord. A sample of this fluid is taken and tested for presence of Lymphoma cells as part of investigations.
Biopsy
A biopsy of the abnormal area in the brain is done to confirm the diagnosis of CNS lymphoma.
Treatment of Primary CNS Lymphoma
The treatment of this condition mainly depends on the age and fitness of the patient.
Chemotherapy
For patients who are young and fit, combination chemotherapy is the treatment of choice for this condition. This chemotherapy includes drugs such as Methotrexate, Cytarabine and Rituximab. This treatment can cause a lot of side effects and hence only given in this group of patients. For patients who have a complete response to treatment, no further treatment may be needed. On the other hand, some doctors advise treatment such as stem cell transplant or radiotherapy or consolidation chemotherapy. A course of chemotherapy may also be given into the spinal canal and is called as intrathecal chemotherapy.
For patients that are not fit or are aged more than 50 years, less intensive chemotherapy such as Temozolomide and Rituximab are used to treat the disease.
Radiotherapy
Radiotherapy is an option of treatment for patients with this condition. Radiotherapy is not a curative treatment on its own. Radiotherapy is usually an option of treatment in patients who do not have a complete response to chemotherapy, are not fit enough to have chemotherapy or have recurrence of the cancer after chemotherapy. The course of radiotherapy ranges from 3-5 weeks depending on the situation that it is being used in.
Bone marrow transplant or stem cell transplant is a type of treatment used in Non-Hodgkin lymphoma when the cancer has come back (relapsed) after initial treatment or the disease does not go away with initial chemotherapy.
Prior to having a bone marrow transplant, the patient is given a high dose of chemotherapy, for example a regimen of chemotherapy like BEAM. The aim of this chemotherapy is to kill off all lymphoma cells. As this chemotherapy is high dose, it kills off normal cells present in the bone marrow also.
The function of the bone marrow normally is to produce blood cells such as red blood cells which help the blood to carry oxygen, white blood cells which protect against infections and platelets which help stop bleeding. A significant lowering of these cells in the blood is dangerous to the patient and hence a transplant of these cells is needed after a high dose of chemotherapy.
Collection of Stem Cells
Stem cells are a type of blood cells that have the capacity to develop into any kind of blood cell such as red blood, white blood cell or platelets. These stem cells are present in the blood stream and bone marrow and are initially collected from the patient before the patient receives high dose chemotherapy. This process of collection of stem cells from the patient and infusing them back into the same patient after high dose chemotherapy is called as Autologous Stem cell transplant.
If the stem cells are from another person(donor), then it is called an Allogenic stem cell transplant. The donor can be related, usually a brother or a sister, or unrelated but matched donor. A donor may be used in situations when there is cancer present in the marrow or an Autologous transplant was done before, but the disease has relapsed again.
Before collection of stem cells, the patient may have chemotherapy and injections with G-CSF which will increase the number of stem cells in the blood to achieve a successful collection.
On the day of collection of stem cells, the patient is connected to a machine and the patient’s blood is taken out from one vein and it passes through the machine to collect the stem cells present in the blood. The blood then passes back into the patient through another vein. This process is done over a few hours.
Once the stem cells are collected, the patient receives the high dose chemotherapy. After the chemotherapy, the stem cells are infused back into the patient. These cells go into the bone marrow and start making blood cells again.
Stem cell transplant is more commonly used these days as compared to bone marrow transplant.
Collection of bone marrow
Bone marrow is the spongy material that is present inside the bones. For a bone marrow transplant, the marrow needs to be collected prior to giving high dose chemotherapy. The procedure to collect the marrow is done under general anaesthesia usually in an operation theatre. The marrow may be taken out from different places in the bones and about 1 litre of it may be taken out at the procedure. Once taken out, it is stored and infused into the patient when needed.
Risks and side effects of Stem cell and Bone marrow Transplant
Having a stem cell or bone marrow transplant is a complex process and is associated with side effects. This procedure usually involves staying in hospital for a few weeks for the blood cells in the marrow and blood to recover to normal levels after the transplant is done. Common side effects associated with this procedure include
Nausea, Vomiting, Hair loss, altered function of the liver are potential side effects of this treatment.
Risk of Infection as white blood cells are low and the patient to prone to get an infection. The infections could be bacterial, viral or fungal and will usually need antibiotics to control them.
Mucositis is due to the effect of chemotherapy on the inside lining of the mouth and digestive tract. This can limit the amount of food taken by the patient and other methods of feeding may be used in that instance.
Bleeding is a risk associated with this procedure due to low platelet count, but platelet transfusion can be given to keep the platelet counts up.
Graft versus host disease This is a reaction of the body to the transfused cells particularly if the stem cells or marrow is from a donor.
